Bones of Lower limb
Region---------------------------------------------Bones
Gluteal -------------------------------------------Hip bone, Sacrum, Coccyx
Thigh-----------------------------------------------Femur, Patella
Leg ------------------------------------------------ Tibia, Fibula
Foot------------------------------------------------Tarsal bones
1)Talus 2) Calcaneus 3) Navicular 4) Medial cuneiform 5) Intermediate cuneiform 6) Lateral cuneiform 7) Cuboid
Metatarsals 5
Phalanges 14 (2-3-3-3-3 mediolaterally)
Region---------------------------------------------Bones
Gluteal -------------------------------------------Hip bone, Sacrum, Coccyx
Thigh-----------------------------------------------Femur, Patella
Leg ------------------------------------------------ Tibia, Fibula
Foot------------------------------------------------Tarsal bones
1)Talus 2) Calcaneus 3) Navicular 4) Medial cuneiform 5) Intermediate cuneiform 6) Lateral cuneiform 7) Cuboid
Metatarsals 5
Phalanges 14 (2-3-3-3-3 mediolaterally)
HIP
Hip bone is irregular bone. It shows two expanded parts and a centraly placed depression acetabulum. It articulates with sacrum posteriorly and with opposite hip bone anteriorly.
Parts
Ilium
Ischium
Pubis
Acetabulum
Ilium
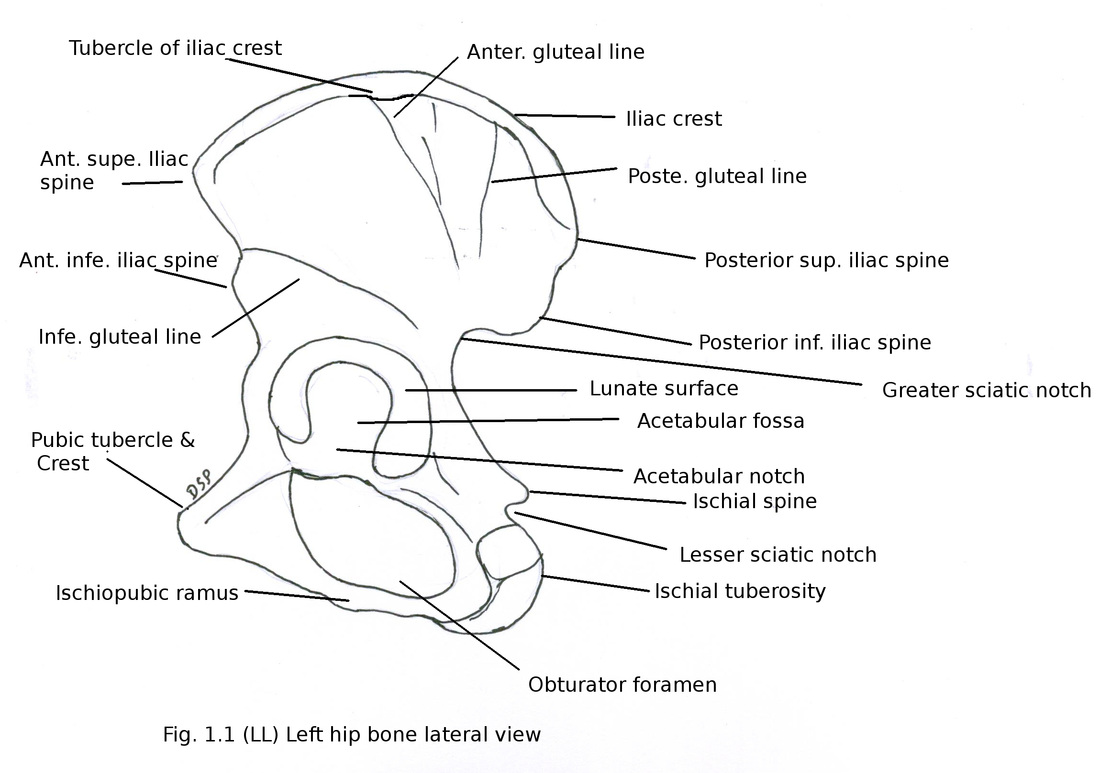
It is upper expanded part. It shows upper and lower ends, three borders anterior, posterior, medial and three surfaces iliac fossa, gluteal surface, sacropelvic surface.
Upper end shows iliac crest from anterior superior iliac spine to posterior superior iliac spine. It is concavocovex on outer aspect antero-posteriorly. It shows two segments ventral 2/3 rd and dorsal 1/3rd. Ventral segment shows outer lip, inner lip and an intermediate area. On outer lip 5cm from anterior superior iliac spine there is presence of tubercle of iliac crest. Dorsal segment shows outer and inner surfaces divided by a line.
Lower end joins with ischium and pubis in the floor of acetabulum.
Anterior border extends from anterior superior iliac spine in upper part to acetabulum. It shows a concave part just below anterior superior iliac spine. In lower part shows small projection as anterior inferior iliac spine.
Posterior border extends from posterior superior iliac spine in upper part to posterior inferior iliac spine in lower part. Then it forms upper margin of greater sciatic notch continue with lower margin of greater sciatic notch to join margin of ischial spine below.
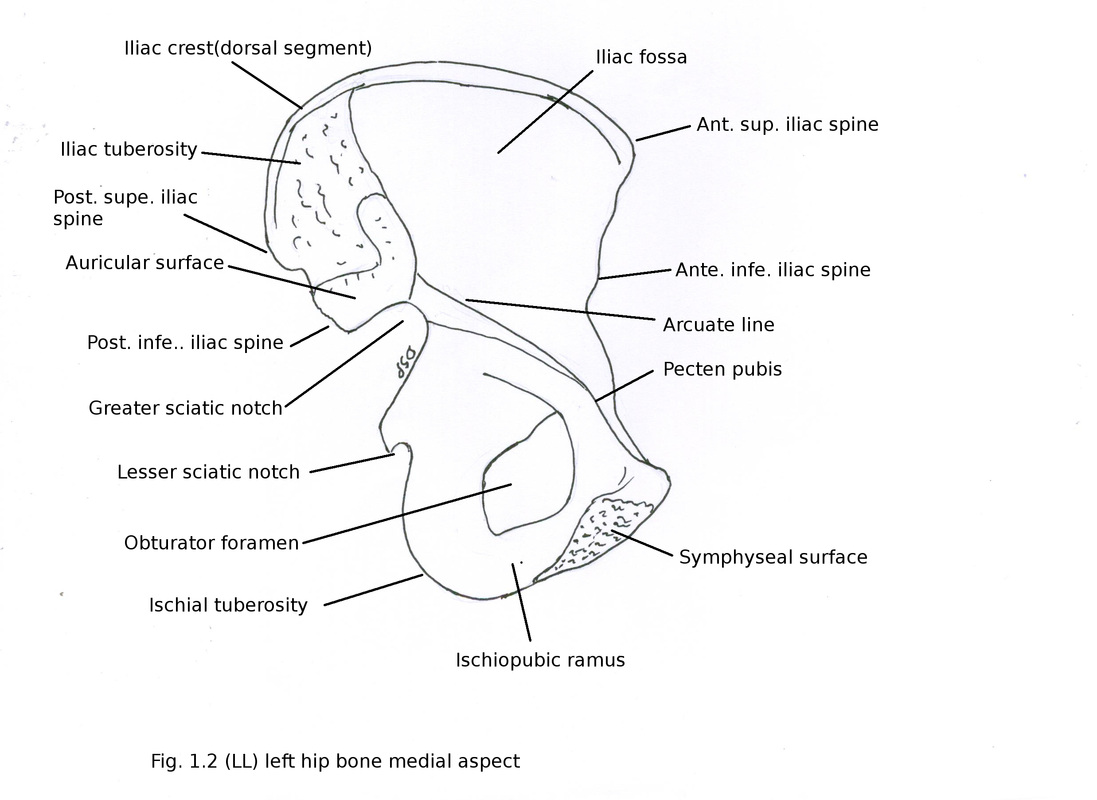
Medial border extends from iliac crest in posterior part. It goes downwards and forwards on medial aspect. It separate iliac fossa and sacropelvic surface. It is rough in upper part, shows sharp margin in middle and smooth and round in lower part. It forms part of arcuate line.
Iliac fossa is a concave surface present on inner aspect of hip bone. Anteriorly bounded by anterior border, posteriorly by medial border above limited by iliac crest.
Gluteal surface is present on outer aspect of hip bone below iliac crest. It shows three gluteal lines. Anterior gluteal line extends from upper margin of greater sciatic notch goes forwards and up to tubercle of iliac crest. Posterior gluteal line extends from upper margin of greater sciatic notch goes to iliac crest 5cm in front of posterior part of iliac crest. Inferior gluteal line extends from upper margin of near apex of greater sciatic notch goes to anterior inferior iliac spine. So gluteal surface is divided into four areas by three gluteal lines.
Sacropelvic surface is between medial border and posterior border. It shows auricular surface, iliac tuberosity, pelvic surface.
Auricular surface shows articulation with lateral part of sacrum forming sacroiliac joint. Iliac tuberosity is a large area present on posterior part of iliac crest. Iliac tuberosity is divided into two areas by an oblique ridge. Pelvic surface is smooth. Arcuate line separates it from iliac fossa. It forms lateral wall of lesser pelvis in lower aspect.
Ischium
It shows body and ramus. It shows two ends upper and lower, three surfaces femoral, posterior and pelvic and three borders anterior, posterior, lateral.
Anterior border is posterior border of obturator foramen.
Posterior border is a cotinuation of posterior border of ilium. A ischial spine is present on posterior border divides it into greater and lesser sciatic notch above and below.
Lateral border is present just below acetabulum laterally and continue with lateral border of ischial tuberosity.
Femoral (Anterior) surface present anteriorly facing downwards and laterally.
Posterior surface present posteriorly and continuous with gluteal surface of ilium.
Pelvic surface present medially inside pelvis.
Ramus of ischium goes upwards and medially from body to join with inferior ramus of pubis and forms ischio-pubic ramus. It shows anterior and posterior surfaces, medial and lateral borders.
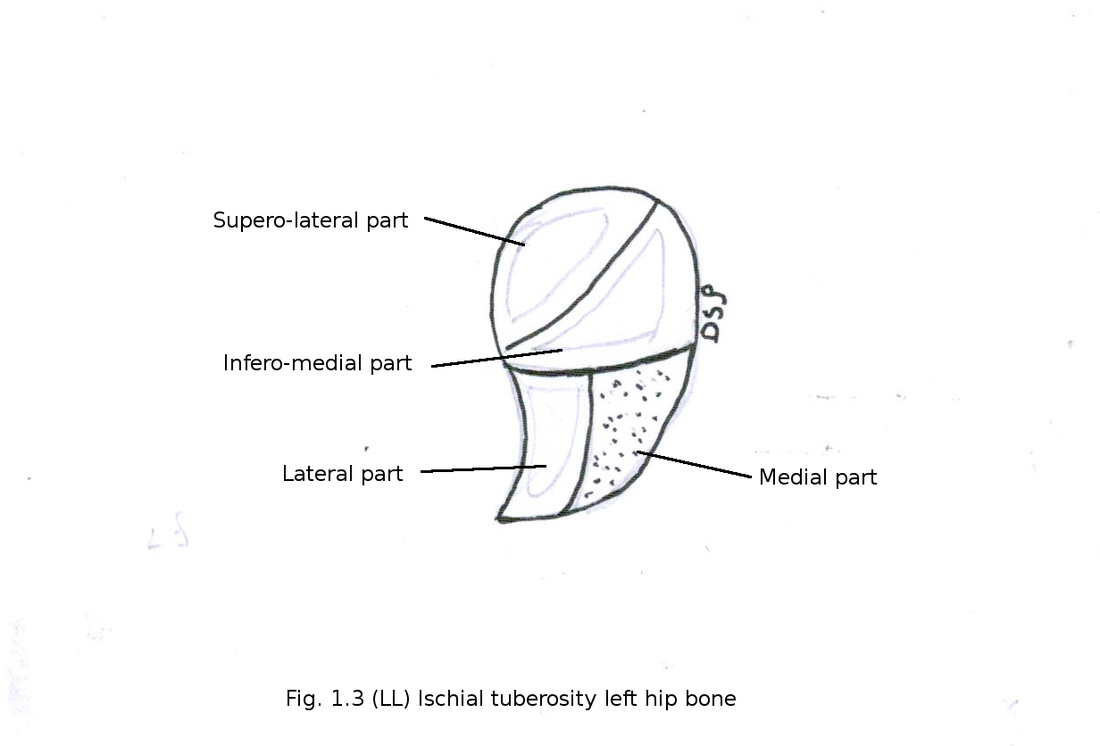
Ischial tuberosity is present on lower aspect of body. It is divided into upper and lower areas by a transverse line. Upper area is again divided by an oblique line into superolateral and inferomedial area. Lower area divided by a verticle line into medial and lateral areas.
Pubis
It shows body and two ramus superior and inferior ramus.
Body shows anterior surface, posterior surface and medial surface.
Anterior surface directed inferolaterally.
Posterior surface forms part of wall of lesser pelvis.
Medial surface joins with opposite medial surface and forms pubic symphysis. A pubic tubercle and pubic crest present on upper part of body near pubic symphysis.
Superior ramus goes upward, backward and laterally. It shows three surfaces anterior (obturator), posterior (pelvic) and superior (pectineal). It shows three borders anterior, posterior and inferior. Anterior border forms pubic crest and goes upto acetabulum.
Posterior border forms part of pectineal line.
Inferior border forms part of obturator foramen.
Anterior surface shows a obturator canal in upper part transmiting obturator nerve, artery and vein. Anterior surface faces anterolaterally.
Posterior surface faces on inner aspect forming part of pelvis.
Pectineal surface formed between anterior and posterior borders in upper part.
Inferior ramus goes downwards and laterally to join with ramus of ischium.
Acetabulum
It is a rounded cavity on lateral part of hip bone. It shows an irregular margin (lunate surface) which is deficient inferiorly and forms acetabular notch. Remaining cavity forms acetabular fossa containing fat. Acetabulum formation is as follows pubis 1/5th, ilium 2/5th and ischium 2/5th part.
Obturator foramen
It is formed by contribution of superiorly by superior pubic ramus and body of pubis inferomedially by inferior ramus of pubis and ramus of ischium, laterally by ischium body and acetabular margin. It is triangular or oval in female and male respectively.
Normal anatomical position
It is as follows anterior superior iliac spine and upper part of pubic symphysis lies in same coronal plane.
Hip bone is irregular bone. It shows two expanded parts and a centraly placed depression acetabulum. It articulates with sacrum posteriorly and with opposite hip bone anteriorly.
Parts
Ilium
Ischium
Pubis
Acetabulum
Ilium
It is upper expanded part. It shows upper and lower ends, three borders anterior, posterior, medial and three surfaces iliac fossa, gluteal surface, sacropelvic surface.
Upper end shows iliac crest from anterior superior iliac spine to posterior superior iliac spine. It is concavocovex on outer aspect antero-posteriorly. It shows two segments ventral 2/3 rd and dorsal 1/3rd. Ventral segment shows outer lip, inner lip and an intermediate area. On outer lip 5cm from anterior superior iliac spine there is presence of tubercle of iliac crest. Dorsal segment shows outer and inner surfaces divided by a line.
Lower end joins with ischium and pubis in the floor of acetabulum.
Anterior border extends from anterior superior iliac spine in upper part to acetabulum. It shows a concave part just below anterior superior iliac spine. In lower part shows small projection as anterior inferior iliac spine.
Posterior border extends from posterior superior iliac spine in upper part to posterior inferior iliac spine in lower part. Then it forms upper margin of greater sciatic notch continue with lower margin of greater sciatic notch to join margin of ischial spine below.
Medial border extends from iliac crest in posterior part. It goes downwards and forwards on medial aspect. It separate iliac fossa and sacropelvic surface. It is rough in upper part, shows sharp margin in middle and smooth and round in lower part. It forms part of arcuate line.
Iliac fossa is a concave surface present on inner aspect of hip bone. Anteriorly bounded by anterior border, posteriorly by medial border above limited by iliac crest.
Gluteal surface is present on outer aspect of hip bone below iliac crest. It shows three gluteal lines. Anterior gluteal line extends from upper margin of greater sciatic notch goes forwards and up to tubercle of iliac crest. Posterior gluteal line extends from upper margin of greater sciatic notch goes to iliac crest 5cm in front of posterior part of iliac crest. Inferior gluteal line extends from upper margin of near apex of greater sciatic notch goes to anterior inferior iliac spine. So gluteal surface is divided into four areas by three gluteal lines.
Sacropelvic surface is between medial border and posterior border. It shows auricular surface, iliac tuberosity, pelvic surface.
Auricular surface shows articulation with lateral part of sacrum forming sacroiliac joint. Iliac tuberosity is a large area present on posterior part of iliac crest. Iliac tuberosity is divided into two areas by an oblique ridge. Pelvic surface is smooth. Arcuate line separates it from iliac fossa. It forms lateral wall of lesser pelvis in lower aspect.
Ischium
It shows body and ramus. It shows two ends upper and lower, three surfaces femoral, posterior and pelvic and three borders anterior, posterior, lateral.
Anterior border is posterior border of obturator foramen.
Posterior border is a cotinuation of posterior border of ilium. A ischial spine is present on posterior border divides it into greater and lesser sciatic notch above and below.
Lateral border is present just below acetabulum laterally and continue with lateral border of ischial tuberosity.
Femoral (Anterior) surface present anteriorly facing downwards and laterally.
Posterior surface present posteriorly and continuous with gluteal surface of ilium.
Pelvic surface present medially inside pelvis.
Ramus of ischium goes upwards and medially from body to join with inferior ramus of pubis and forms ischio-pubic ramus. It shows anterior and posterior surfaces, medial and lateral borders.
Ischial tuberosity is present on lower aspect of body. It is divided into upper and lower areas by a transverse line. Upper area is again divided by an oblique line into superolateral and inferomedial area. Lower area divided by a verticle line into medial and lateral areas.
Pubis
It shows body and two ramus superior and inferior ramus.
Body shows anterior surface, posterior surface and medial surface.
Anterior surface directed inferolaterally.
Posterior surface forms part of wall of lesser pelvis.
Medial surface joins with opposite medial surface and forms pubic symphysis. A pubic tubercle and pubic crest present on upper part of body near pubic symphysis.
Superior ramus goes upward, backward and laterally. It shows three surfaces anterior (obturator), posterior (pelvic) and superior (pectineal). It shows three borders anterior, posterior and inferior. Anterior border forms pubic crest and goes upto acetabulum.
Posterior border forms part of pectineal line.
Inferior border forms part of obturator foramen.
Anterior surface shows a obturator canal in upper part transmiting obturator nerve, artery and vein. Anterior surface faces anterolaterally.
Posterior surface faces on inner aspect forming part of pelvis.
Pectineal surface formed between anterior and posterior borders in upper part.
Inferior ramus goes downwards and laterally to join with ramus of ischium.
Acetabulum
It is a rounded cavity on lateral part of hip bone. It shows an irregular margin (lunate surface) which is deficient inferiorly and forms acetabular notch. Remaining cavity forms acetabular fossa containing fat. Acetabulum formation is as follows pubis 1/5th, ilium 2/5th and ischium 2/5th part.
Obturator foramen
It is formed by contribution of superiorly by superior pubic ramus and body of pubis inferomedially by inferior ramus of pubis and ramus of ischium, laterally by ischium body and acetabular margin. It is triangular or oval in female and male respectively.
Normal anatomical position
It is as follows anterior superior iliac spine and upper part of pubic symphysis lies in same coronal plane.
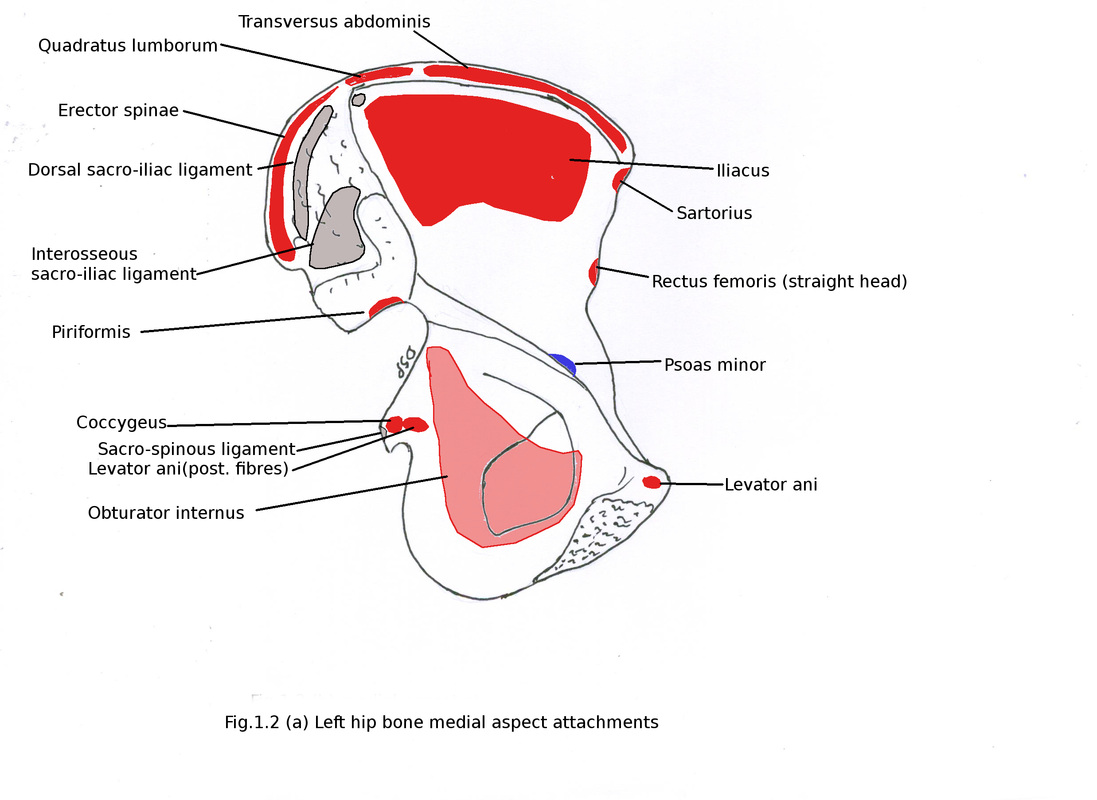
Attachments
Ilium
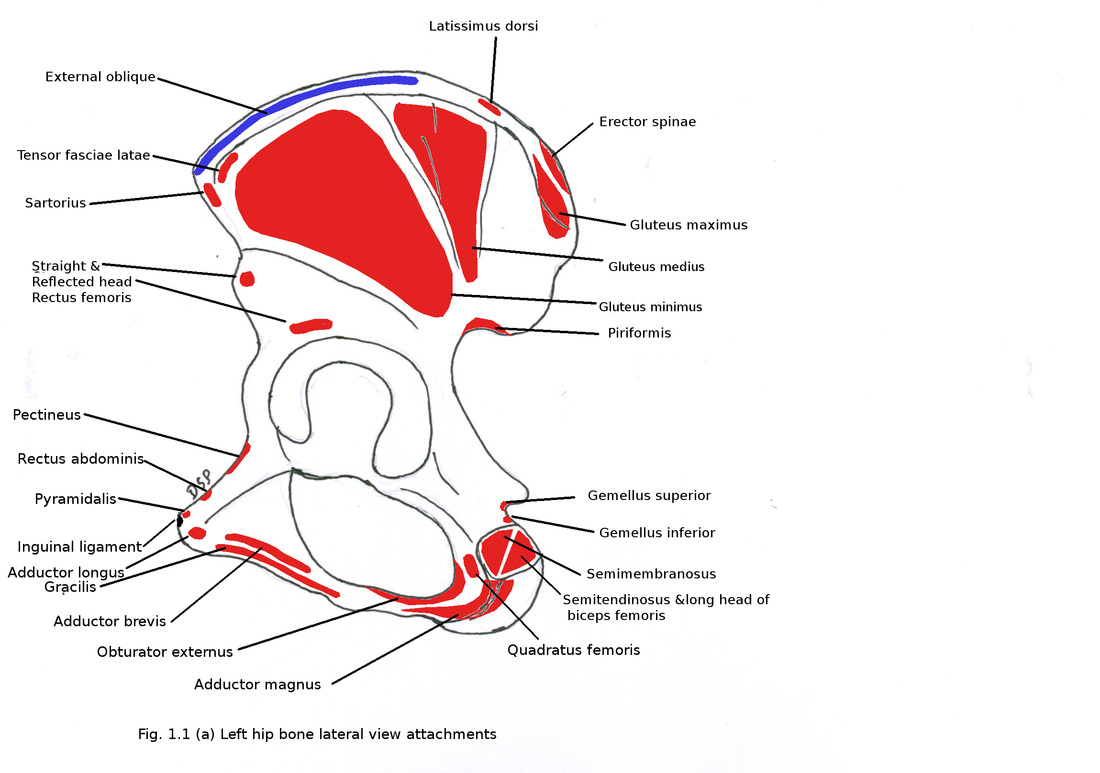
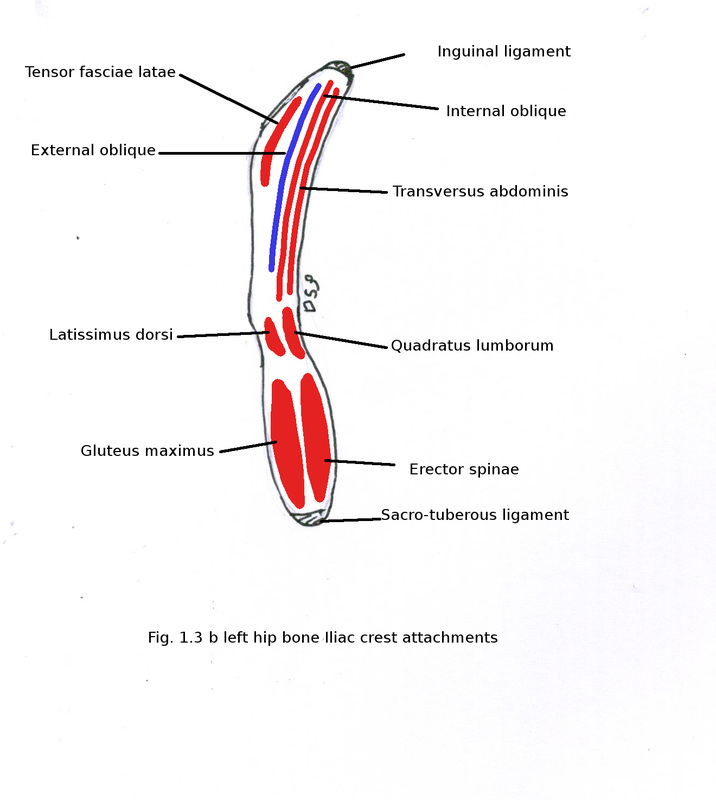
Iliac crest shows attachment on its ventral segment from lateral to medially. On outer lip fascia lata alongwith iliotibial tract, insertion of external oblique muscle on anterior 2/3rd part, latissimus dorsi just posterior to it.
On intermediate area shows attachment of internal oblique.
On lateral lip shows attachment of transversus abdominis anterior 2/3rd part, quadratus lumborum on posterior 1/3 rd part, facscia transversalis, fascia iliaca.
Dorsal segment of iliac crest shows origin of gluteus maximus on its outer surface and origin of erector spinae on inner surface. In between these two muscles gives attachment to thoracolumbar fascia.
Anterior superior iliac spine shows attachment of lateral end of inguinal ligament. Just below anterior superior iliac spine shows attachment of sartorius.
Anterior inferior iliac spine shows origin of straight head of rectus femoris.
Posterior inferior iliac spine alongwith posterior border upper part shows attchment of sacrotuberous ligament. Part of piriformis shows origin from part anterior to posterior superior iliac spine.
Greater sciatic notch get converted into greater sciatic foramen by sacrotuberous and sacrospinous ligament. Structures which passes through foramen from above downwards superior gluteal vessels and nerves, piriformis muscle, below piriformis structures arranged from lateral to medial side as follows sciatic nerve and nerve to quadratus femoris, posterior femoral cutaneous nerve, inferior gluteal nerve and vessels, nerve to obturator internus, internal pudendal vessels, pudendal nerve.
Medial border on its rough part shows attchment of dorsal sacroiliac ligament and ilio-lumbar ligament. Fascia iliaca and parietal layer of pelvic fascia shows attchment on medial border.
Gluteal surface behind posterior gluteal line shows origin of upper part of gluteus maximus and part of sacrotuberous ligament. Between anterior and posterior gluteal lines shows origin of gluteus medius. Between anterior and inferior gluteal lines shows origin of gluteus minimus. Below inferior gluteal line and above acetabulum shows origin of reflected head of rectus femoris.
On sacropelvic surface iliac tuberosity shows attachment of ilio-lumbar, dorsal sacro-iliac, interosseous sacro-iliac ligaments.
Pelvic surface shows origin of obturator internus in its maximum part but in upper small area shows origin of some fibres of piriformis.
Ischium
Anterior border shows attachment of obturator membrane.
Ischial spine present on posterior border shows attachment of sacrospinous ligament on its tip. Coccygeus and posterior fibres of levator ani shows origin on pelvic surface of spine.
Dorsal surface of spine shows origin of gemellus superior. Gemellus inferior shows origin from lower margin of lesser sciatic notch.
Lesser sciatic foramen is formed by sacrotuberous and sacrospinous ligaments over lesser sciatic foramen. Structures passing through this foramen are tendon of obturator internus, nerve to obturator internus, internal pudendal nerve and internal pudendal vessels.
Lateral border shows attachment of ischio-femoral ligament.
Femoral (Anterior) surface shows origin of obturator externus.
Pelvic surface of ischium shows origin of obturator internus.
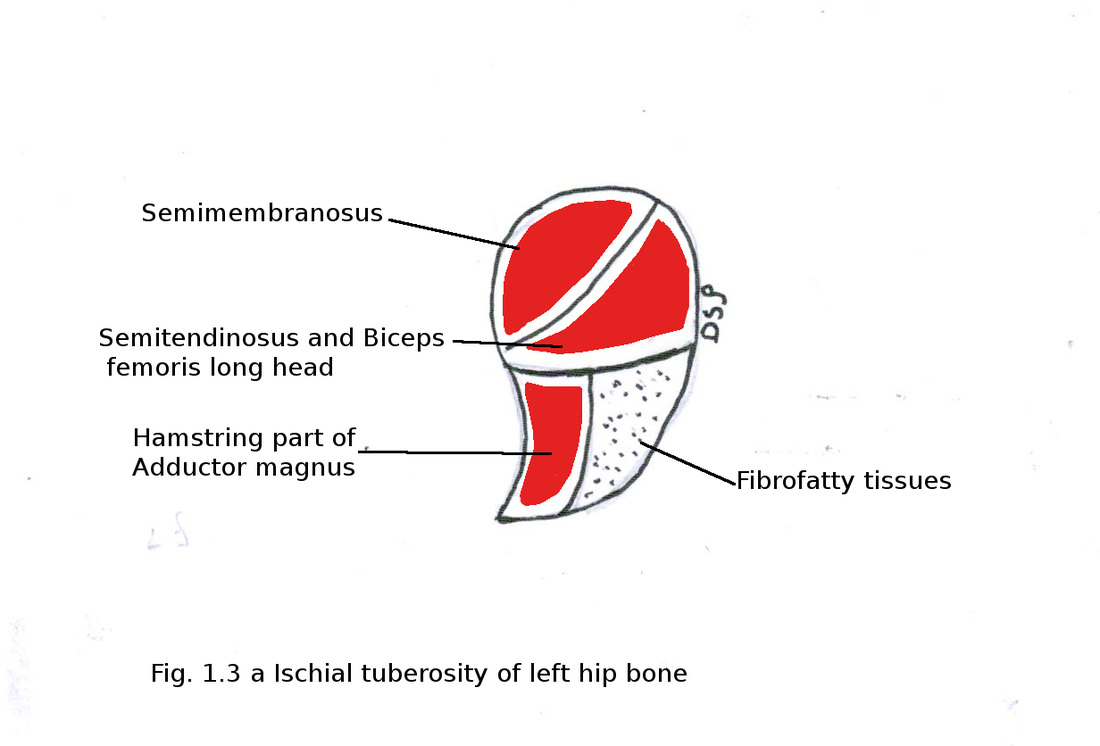
Laterally on ischial tuberosity shows origin of quadratus femoris. Ischial tuberosity upper area superolateral part part shows origin of semimembranosus and inferomedial part shows origin of semitendinosus and long head of biceps femoris. Lower area lateral part shows origin of hamstring part of adductor magnus and medial part with fibrofatty tissues and attachment of sacrotuberous ligament.
Ramus of ischium medial border shows attachment of obturator membrane.
Lateral border shows attachment of superficial perineal fascia, fascia lata.
Anterior surface shows origin of adductor magnus, adductor brevis, gracilis and obturator externus. Posterior surfaces shows attachment of superior and inferior fascia of urogenital diaphragm, crus of penis or clitoris. It also shows origin of obturator internus, sphincter urethrae, transversus perinei profundus, ischio-cavernosus, transversus perinei superficialis.
Pubis
Anterior surface of body shows origin of adductor longus, gracilis, adductor brevis and obturator externus.
Posterior surface shows origin of obturator internus and levator ani anterior fibres.
Pubic tubercle shows attachment of medial end of inguinal ligament, lateral crus of superficial inguinal ring, apex of lacunar ligament, reflected part of inguinal ligament, cremaster muscle in male, superior crus of saphenous opening.
Pubic crest shows attachment of fascia transversalis, fascia lata, rectus sheath anterior wall, conjoint tendon and origin of muscles lateral head of rectus abdominis and pyramidalis.
Superior (pectineal) surface of superior ramus shows origin of pectineus muscle. It shows attchment of pubo-femoral ligament from anterior border.
Inferior border shows attachment of obturator membrane.
Acetabulum
Acetabular labrum present is a fibrocartilagenous rim on margin (lunate surface) of acetabulum.
Ossification:
It ossifies from three primary centres. Primary centre one for ilium, one for body of ischium, one for body of pubis appear in 8th or 9th week, 4th month, 4th to 5th month of intrauterine life.
Secondary centres and time of appearance :
1- two for iliac crest, 2- one for junction of three parts of hip bone as cartilage line in cavity of acetabulum, 3- one for medial surface of pubic symphysis, 4-one for anterior inferior iliac spine, 5- one for ischial tuberosity appears all at puberty. These fuse with each other to form complete bone during 15-25 years.
Formation of ischio-pubic ramus takes place at about 7th or 8th year.
Ilium
Iliac crest shows attachment on its ventral segment from lateral to medially. On outer lip fascia lata alongwith iliotibial tract, insertion of external oblique muscle on anterior 2/3rd part, latissimus dorsi just posterior to it.
On intermediate area shows attachment of internal oblique.
On lateral lip shows attachment of transversus abdominis anterior 2/3rd part, quadratus lumborum on posterior 1/3 rd part, facscia transversalis, fascia iliaca.
Dorsal segment of iliac crest shows origin of gluteus maximus on its outer surface and origin of erector spinae on inner surface. In between these two muscles gives attachment to thoracolumbar fascia.
Anterior superior iliac spine shows attachment of lateral end of inguinal ligament. Just below anterior superior iliac spine shows attachment of sartorius.
Anterior inferior iliac spine shows origin of straight head of rectus femoris.
Posterior inferior iliac spine alongwith posterior border upper part shows attchment of sacrotuberous ligament. Part of piriformis shows origin from part anterior to posterior superior iliac spine.
Greater sciatic notch get converted into greater sciatic foramen by sacrotuberous and sacrospinous ligament. Structures which passes through foramen from above downwards superior gluteal vessels and nerves, piriformis muscle, below piriformis structures arranged from lateral to medial side as follows sciatic nerve and nerve to quadratus femoris, posterior femoral cutaneous nerve, inferior gluteal nerve and vessels, nerve to obturator internus, internal pudendal vessels, pudendal nerve.
Medial border on its rough part shows attchment of dorsal sacroiliac ligament and ilio-lumbar ligament. Fascia iliaca and parietal layer of pelvic fascia shows attchment on medial border.
Gluteal surface behind posterior gluteal line shows origin of upper part of gluteus maximus and part of sacrotuberous ligament. Between anterior and posterior gluteal lines shows origin of gluteus medius. Between anterior and inferior gluteal lines shows origin of gluteus minimus. Below inferior gluteal line and above acetabulum shows origin of reflected head of rectus femoris.
On sacropelvic surface iliac tuberosity shows attachment of ilio-lumbar, dorsal sacro-iliac, interosseous sacro-iliac ligaments.
Pelvic surface shows origin of obturator internus in its maximum part but in upper small area shows origin of some fibres of piriformis.
Ischium
Anterior border shows attachment of obturator membrane.
Ischial spine present on posterior border shows attachment of sacrospinous ligament on its tip. Coccygeus and posterior fibres of levator ani shows origin on pelvic surface of spine.
Dorsal surface of spine shows origin of gemellus superior. Gemellus inferior shows origin from lower margin of lesser sciatic notch.
Lesser sciatic foramen is formed by sacrotuberous and sacrospinous ligaments over lesser sciatic foramen. Structures passing through this foramen are tendon of obturator internus, nerve to obturator internus, internal pudendal nerve and internal pudendal vessels.
Lateral border shows attachment of ischio-femoral ligament.
Femoral (Anterior) surface shows origin of obturator externus.
Pelvic surface of ischium shows origin of obturator internus.
Laterally on ischial tuberosity shows origin of quadratus femoris. Ischial tuberosity upper area superolateral part part shows origin of semimembranosus and inferomedial part shows origin of semitendinosus and long head of biceps femoris. Lower area lateral part shows origin of hamstring part of adductor magnus and medial part with fibrofatty tissues and attachment of sacrotuberous ligament.
Ramus of ischium medial border shows attachment of obturator membrane.
Lateral border shows attachment of superficial perineal fascia, fascia lata.
Anterior surface shows origin of adductor magnus, adductor brevis, gracilis and obturator externus. Posterior surfaces shows attachment of superior and inferior fascia of urogenital diaphragm, crus of penis or clitoris. It also shows origin of obturator internus, sphincter urethrae, transversus perinei profundus, ischio-cavernosus, transversus perinei superficialis.
Pubis
Anterior surface of body shows origin of adductor longus, gracilis, adductor brevis and obturator externus.
Posterior surface shows origin of obturator internus and levator ani anterior fibres.
Pubic tubercle shows attachment of medial end of inguinal ligament, lateral crus of superficial inguinal ring, apex of lacunar ligament, reflected part of inguinal ligament, cremaster muscle in male, superior crus of saphenous opening.
Pubic crest shows attachment of fascia transversalis, fascia lata, rectus sheath anterior wall, conjoint tendon and origin of muscles lateral head of rectus abdominis and pyramidalis.
Superior (pectineal) surface of superior ramus shows origin of pectineus muscle. It shows attchment of pubo-femoral ligament from anterior border.
Inferior border shows attachment of obturator membrane.
Acetabulum
Acetabular labrum present is a fibrocartilagenous rim on margin (lunate surface) of acetabulum.
Ossification:
It ossifies from three primary centres. Primary centre one for ilium, one for body of ischium, one for body of pubis appear in 8th or 9th week, 4th month, 4th to 5th month of intrauterine life.
Secondary centres and time of appearance :
1- two for iliac crest, 2- one for junction of three parts of hip bone as cartilage line in cavity of acetabulum, 3- one for medial surface of pubic symphysis, 4-one for anterior inferior iliac spine, 5- one for ischial tuberosity appears all at puberty. These fuse with each other to form complete bone during 15-25 years.
Formation of ischio-pubic ramus takes place at about 7th or 8th year.
FEMUR
Parts of Femur :
Upper end
Shaft
Lower end
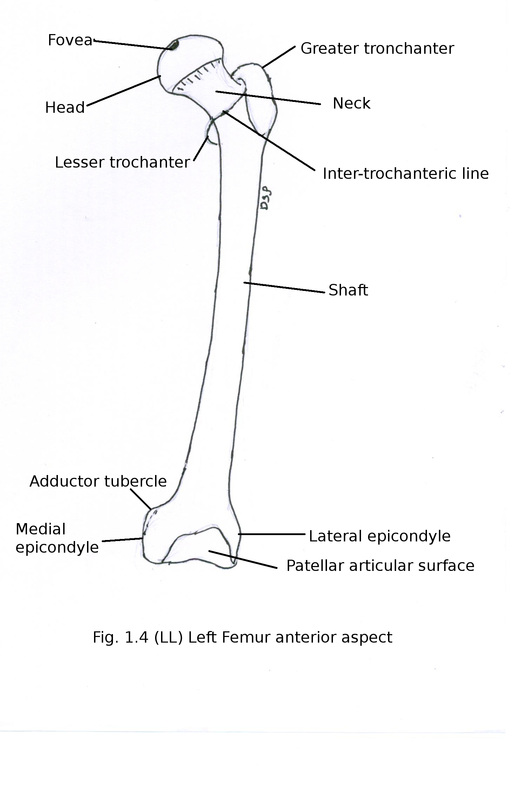
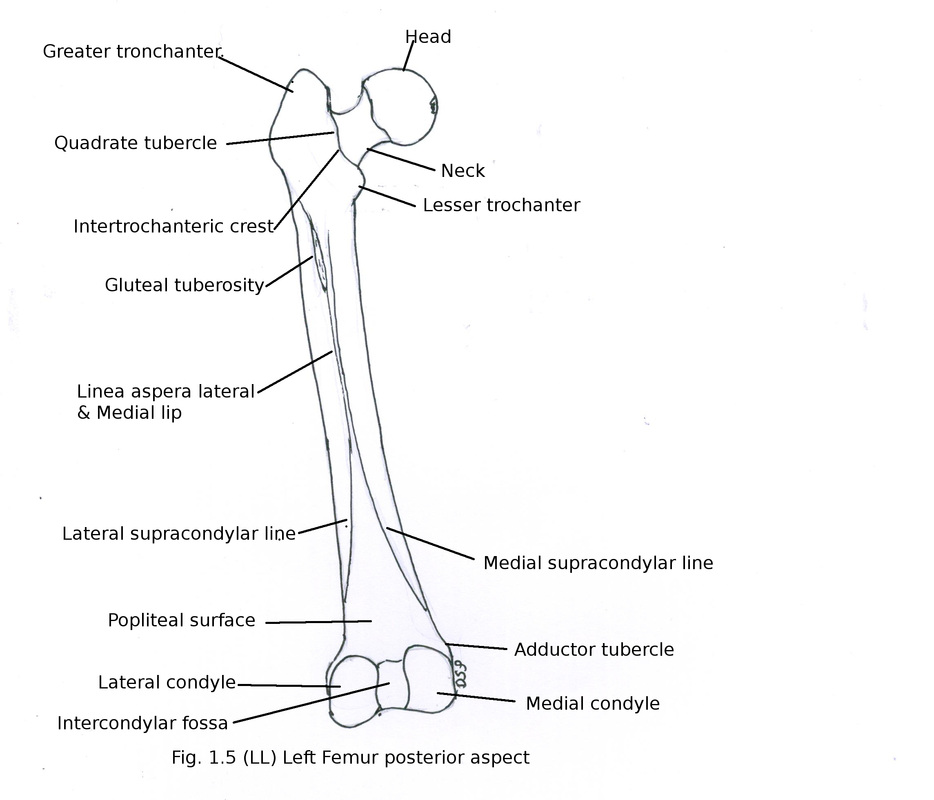
Upper end
It shows head, neck, greater trochanter, lesser trochanter, inter-trochantric line, inter-trochantric crest.
Head is rounded forming more than half part is articular. It shows a small depression in the centre named pit or fovea. It articulates with acetabulum of hip bone forming hip joint.
Neck is long directed medially, forwards and upwards. Neck shaft angle is 135 degree in adult to increase range of movements at hip joint.
Upper margin of neck concave but horizontally placed.
Lower margin is oblique but straight. On posterior surface a groove present for tendon of obturator externus. It is convex medio-laterally and concave from below upwards. Anterior surface is flat with transverse lines for attachment of capsule.
Greater trochanter is a quadrangular projection going upwards. It is part of upper end. It shows three surfaces medial, lateral, anterior and two borders superior, posterior. Medial surface shows trochantric fossa. Lateral surface square shaped divided by an elevated line which goes downwards and anteriorly into upper and lower triangular surfaces.
Lesser trochanter is an elevation on lower part of upper end at junction of neck and shaft postero-medially. It shows anterior surface, posterior surface and tip.
Inter-trochantric line present at upper end of shaft anteriorly between junction of neck and shaft. It goes downwards and medially from greater trochanter to lesser trochanter then continue as spiral line.
Inter-trochantric crest present at upper end of shaft posteriorly between junction of neck and shaft. It goes downwards and medially from posterior superior angle of greater trochanter to lesser trochanter. A quadrate tubercle present on this line.
Shaft
It has three borders posterior, medial, lateral and three surfaces medial, lateral, anterior. It shows slight convexity anteriorly in the middle. Posterior border is rough known as linea aspera. It shows two edges medial and lateral. Linea aspera goes upwards and diverge in upper and posterior part forming a triangular area on shaft. Medial rough edge continue upwards as spiral line. While lateral edge shows gluteal tuberosity. Popliteal trangular surface formed by diverging two edges of linea aspera in lower part of femur. Then medial and lateral edges continue as medial and lateral supracondylar lines. Medial and lateral borders are rounded borders present on medial and lateral apect of shaft. Anterior surface present in between medial and lateral borders. Medial surface is actually posteromedial between medial and posterior borders. Lateral surface is actually posterolateral between lateral and posterior borders.
Lower end
It is large and expanded from side to side. It shows two condyles medial and lateral. It articulates anteriorly with patella. Posteriorly condyles extends and articulates inferiorly and posteriorly with condyles of tibia. An intercondylar fossa present posteriorly in between two condyles. Articular area is having U shape. Prominent elevations present on medial and lateral condyles of femur are medial and lateral epicondyles. Lateral condyle shows a groove just above lateral epicondyle for tendon of popliteus muscle. Intercondylar fossa shows two walls medial and lateral. An adductor tubercle present on medial condyle of in its upper part.
Parts of Femur :
Upper end
Shaft
Lower end
Upper end
It shows head, neck, greater trochanter, lesser trochanter, inter-trochantric line, inter-trochantric crest.
Head is rounded forming more than half part is articular. It shows a small depression in the centre named pit or fovea. It articulates with acetabulum of hip bone forming hip joint.
Neck is long directed medially, forwards and upwards. Neck shaft angle is 135 degree in adult to increase range of movements at hip joint.
Upper margin of neck concave but horizontally placed.
Lower margin is oblique but straight. On posterior surface a groove present for tendon of obturator externus. It is convex medio-laterally and concave from below upwards. Anterior surface is flat with transverse lines for attachment of capsule.
Greater trochanter is a quadrangular projection going upwards. It is part of upper end. It shows three surfaces medial, lateral, anterior and two borders superior, posterior. Medial surface shows trochantric fossa. Lateral surface square shaped divided by an elevated line which goes downwards and anteriorly into upper and lower triangular surfaces.
Lesser trochanter is an elevation on lower part of upper end at junction of neck and shaft postero-medially. It shows anterior surface, posterior surface and tip.
Inter-trochantric line present at upper end of shaft anteriorly between junction of neck and shaft. It goes downwards and medially from greater trochanter to lesser trochanter then continue as spiral line.
Inter-trochantric crest present at upper end of shaft posteriorly between junction of neck and shaft. It goes downwards and medially from posterior superior angle of greater trochanter to lesser trochanter. A quadrate tubercle present on this line.
Shaft
It has three borders posterior, medial, lateral and three surfaces medial, lateral, anterior. It shows slight convexity anteriorly in the middle. Posterior border is rough known as linea aspera. It shows two edges medial and lateral. Linea aspera goes upwards and diverge in upper and posterior part forming a triangular area on shaft. Medial rough edge continue upwards as spiral line. While lateral edge shows gluteal tuberosity. Popliteal trangular surface formed by diverging two edges of linea aspera in lower part of femur. Then medial and lateral edges continue as medial and lateral supracondylar lines. Medial and lateral borders are rounded borders present on medial and lateral apect of shaft. Anterior surface present in between medial and lateral borders. Medial surface is actually posteromedial between medial and posterior borders. Lateral surface is actually posterolateral between lateral and posterior borders.
Lower end
It is large and expanded from side to side. It shows two condyles medial and lateral. It articulates anteriorly with patella. Posteriorly condyles extends and articulates inferiorly and posteriorly with condyles of tibia. An intercondylar fossa present posteriorly in between two condyles. Articular area is having U shape. Prominent elevations present on medial and lateral condyles of femur are medial and lateral epicondyles. Lateral condyle shows a groove just above lateral epicondyle for tendon of popliteus muscle. Intercondylar fossa shows two walls medial and lateral. An adductor tubercle present on medial condyle of in its upper part.
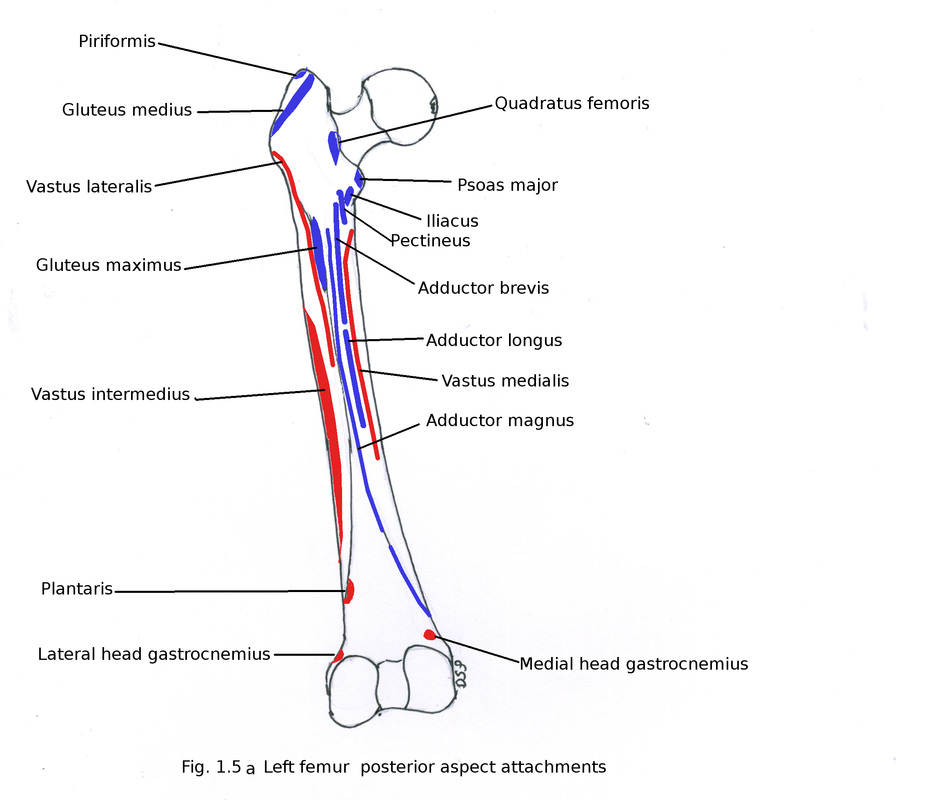
Attachments
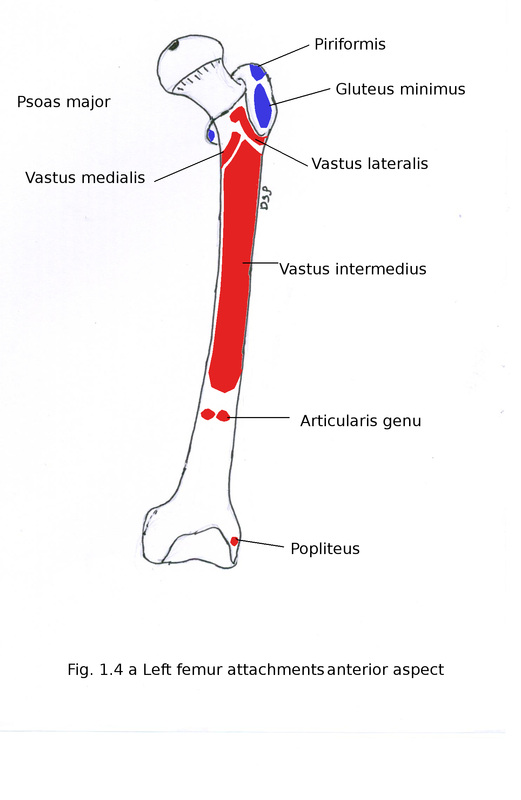
Origin of muscles:
Vastus lateralis shows origin from intertrochantric line, lower part of greater trochanter, lateral margin of gluteal tuberosity and lateral edge of linea aspera.
Vastus medialis shows origin from lower part of intertrochantric line, spiral line and medial edge of linea aspera and upper part of medial supracondylar line.
Vastus intermedius shows origin from anterior surface of shaft upper 3/4th part and from lateral surface.
Articularis genu shows origin from anterior surface lower part of shaft just below origin of vastus intermedius.
Biceps femoris short head shows origin from lateral edge of linea aspera between vastus lateralis and adductor magnus and from upper 2/3rd part of lateral supracondylar line.
Medial head of gastrocnemius shows origin from politeal surface medial part below medial supracondylar line.
Lateral head of gastrocnemius shows origin from lower part of lateral supracondylar line.
Plantaris shows origin from lateral supracondylar line just above origin of lateral head of gastocnemius.
Popliteus shows origin from an area just anterior to groove on lateral condyle of femur below attachment of capsule of knee joint so origin is intracapsular.
Insertion of Muscles:
Gluteus minimus shows insertion on anterior surface of greater trochanter of femur.
Gluteus medius shows insertion on elevated line which goes downwards and anteriorly on greater trochanter.
Obturator externus shows insertion on trochantric fossa on medial aspect of greater trochanter.
Piriformis, gemellus inferior, obturator internus tendon and gemellus superior shows insertion on superior border of greater trochanter from anterior to posterior.
Psoas major tendon shows insertion on tip of lesserr trochanter.
Iliacus shows insertion on base of lesser trochanter on anterior surface.
Quadratus femoris shows insertion on quadrate tubercle present on intertrochantric crest.
Gluteus maximus deep fibres shows partly insertion on gluteal tuberosity.
Adductor brevis and adductor longus shows insertion on area in between medial and lateral edge of linea aspera above and below respectively.
Adductor magnus shows insertion on area in between medial and lateral edge of linea aspera lateral to insertion of adductor brevis and adductor longus below ischial part shows insertion on adductor tubercle .
Iliacus shows insertion on upper triangular area of upper part of shaft.
Pectineus shows insertion on upper triangular area of upper part of shaft lateral to insertion of iliacus.
Other Attachments :
Ligamentum teres shows attachmnt on pit or fovea on head of femur.
Ilio-femoral ligament shows attachment on intertrochantric line.
Capsule of hip joint attached anteriorly on a line medial to intertrochantric line, above upper margin of neck near greater trochanter, below on lower margin of neck just above lesser trochanter, posteriorly on a line medial to intertrochantric crest.
Lateral intermuscular septum shows attachment on lateral edge of linea aspera.
Medial intermuscular septum shows attachment on medial edge of linea aspera.
Posterior intermuscular septum shows attachment on area between medial and lateral edge of linea aspera.
Fibular collateral ligaments shows attachment on lateral epicondyle.
Tibial collateral ligaments shows attachment on medial epicondyle.
Posterior cruciate ligament uppr end shows attachment on medial wall of intercondylar fossa on antero-inferior aspect.
Anterior cruciate ligament uppr end shows attachment on lateral wall of intercondylar fossa on postero-superior aspect.
Capsule of knee joint shows attachment on a line upper margin of intercondylar notch and just above articular margin of medial and lateral condyle.
Ossification:
Femur ossify from 1 primary centre and 4 secondary centres.
1 primary centre for shaft appear during 7th week of intrauterine life.
3 secondary centres for upper end 1-one for head, 2- one for greater trochanter, 3- one for lesser trochanter which appears during 6 to 7th months, 4th year and 14th to 15th year after birth respectively. Fusion takes place of lesser trochanter with shaft in 14 to17th year, greater trochanter in 17 to 18 th year and head in 18 th year.
Lower end ossify from 1centre. It appears in ninth month of intrauterine life. It fuses with shaft after 18th year.
Anatomical position:
Head of femur directed forward, upward and medially. Shaft of femur goes downward and medially.
Applied anatomy:
1. Lower end of femur appears in ninth month of intrauterine life so it is having medicolegal importance. Presence of this centre indicates that child was viable at time of birth.
2. In old age fracture of neck of femur is common.
Origin of muscles:
Vastus lateralis shows origin from intertrochantric line, lower part of greater trochanter, lateral margin of gluteal tuberosity and lateral edge of linea aspera.
Vastus medialis shows origin from lower part of intertrochantric line, spiral line and medial edge of linea aspera and upper part of medial supracondylar line.
Vastus intermedius shows origin from anterior surface of shaft upper 3/4th part and from lateral surface.
Articularis genu shows origin from anterior surface lower part of shaft just below origin of vastus intermedius.
Biceps femoris short head shows origin from lateral edge of linea aspera between vastus lateralis and adductor magnus and from upper 2/3rd part of lateral supracondylar line.
Medial head of gastrocnemius shows origin from politeal surface medial part below medial supracondylar line.
Lateral head of gastrocnemius shows origin from lower part of lateral supracondylar line.
Plantaris shows origin from lateral supracondylar line just above origin of lateral head of gastocnemius.
Popliteus shows origin from an area just anterior to groove on lateral condyle of femur below attachment of capsule of knee joint so origin is intracapsular.
Insertion of Muscles:
Gluteus minimus shows insertion on anterior surface of greater trochanter of femur.
Gluteus medius shows insertion on elevated line which goes downwards and anteriorly on greater trochanter.
Obturator externus shows insertion on trochantric fossa on medial aspect of greater trochanter.
Piriformis, gemellus inferior, obturator internus tendon and gemellus superior shows insertion on superior border of greater trochanter from anterior to posterior.
Psoas major tendon shows insertion on tip of lesserr trochanter.
Iliacus shows insertion on base of lesser trochanter on anterior surface.
Quadratus femoris shows insertion on quadrate tubercle present on intertrochantric crest.
Gluteus maximus deep fibres shows partly insertion on gluteal tuberosity.
Adductor brevis and adductor longus shows insertion on area in between medial and lateral edge of linea aspera above and below respectively.
Adductor magnus shows insertion on area in between medial and lateral edge of linea aspera lateral to insertion of adductor brevis and adductor longus below ischial part shows insertion on adductor tubercle .
Iliacus shows insertion on upper triangular area of upper part of shaft.
Pectineus shows insertion on upper triangular area of upper part of shaft lateral to insertion of iliacus.
Other Attachments :
Ligamentum teres shows attachmnt on pit or fovea on head of femur.
Ilio-femoral ligament shows attachment on intertrochantric line.
Capsule of hip joint attached anteriorly on a line medial to intertrochantric line, above upper margin of neck near greater trochanter, below on lower margin of neck just above lesser trochanter, posteriorly on a line medial to intertrochantric crest.
Lateral intermuscular septum shows attachment on lateral edge of linea aspera.
Medial intermuscular septum shows attachment on medial edge of linea aspera.
Posterior intermuscular septum shows attachment on area between medial and lateral edge of linea aspera.
Fibular collateral ligaments shows attachment on lateral epicondyle.
Tibial collateral ligaments shows attachment on medial epicondyle.
Posterior cruciate ligament uppr end shows attachment on medial wall of intercondylar fossa on antero-inferior aspect.
Anterior cruciate ligament uppr end shows attachment on lateral wall of intercondylar fossa on postero-superior aspect.
Capsule of knee joint shows attachment on a line upper margin of intercondylar notch and just above articular margin of medial and lateral condyle.
Ossification:
Femur ossify from 1 primary centre and 4 secondary centres.
1 primary centre for shaft appear during 7th week of intrauterine life.
3 secondary centres for upper end 1-one for head, 2- one for greater trochanter, 3- one for lesser trochanter which appears during 6 to 7th months, 4th year and 14th to 15th year after birth respectively. Fusion takes place of lesser trochanter with shaft in 14 to17th year, greater trochanter in 17 to 18 th year and head in 18 th year.
Lower end ossify from 1centre. It appears in ninth month of intrauterine life. It fuses with shaft after 18th year.
Anatomical position:
Head of femur directed forward, upward and medially. Shaft of femur goes downward and medially.
Applied anatomy:
1. Lower end of femur appears in ninth month of intrauterine life so it is having medicolegal importance. Presence of this centre indicates that child was viable at time of birth.
2. In old age fracture of neck of femur is common.
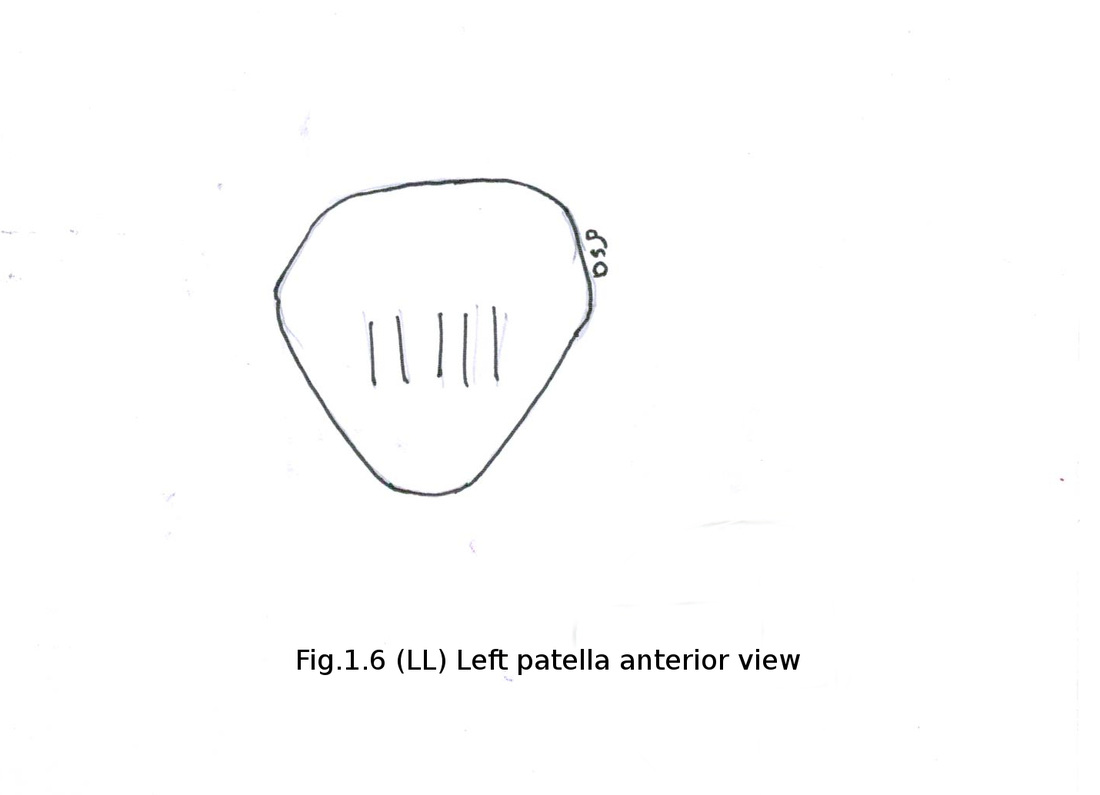
Patella
It is large and big sesamoid bone which ossifies in the tendon of quadriceps femoris muscle.
It is a triangular bone.
It shows an apex, base (upper border), medial and lateral borders and two surface anterior and posterior.
Apex is pointed lower end of patella. Base is upper margin of patella. Medial and lateral borders goes downward towards apex.
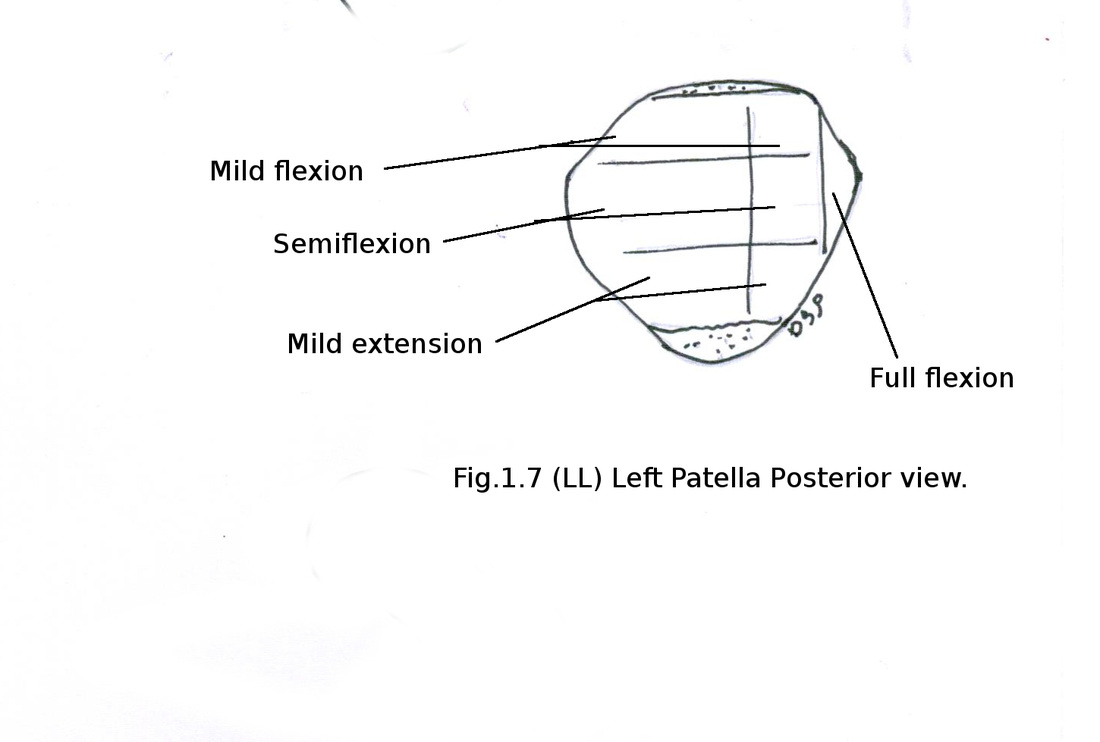
Anterior surface is covered skin only so it is subcutaneous. A pre-patellar bursa present in relation with it. Vertical lines present on this surface. Posterior surface is articular for articulation with lower end of femur but near apex it is nonarticular. It is divided by vertical prominent elevation (ridge) into lateral and medial parts which are large and small respectively. Medial part again divided by a vertical ridge into a small medial segment and large lateral segment. Both large lateral segment (medial part) and lateral part are subdivided by two transverse lines into upper, middle, and lower areas.
Areas which comes in contact with patellar articular area of femur in different positions :
upper area - during mild flexion
middle area - during semiflexion
lower area – during mild extension
medial area – during full flexion
During full extension patella floats anterior to knee joint.
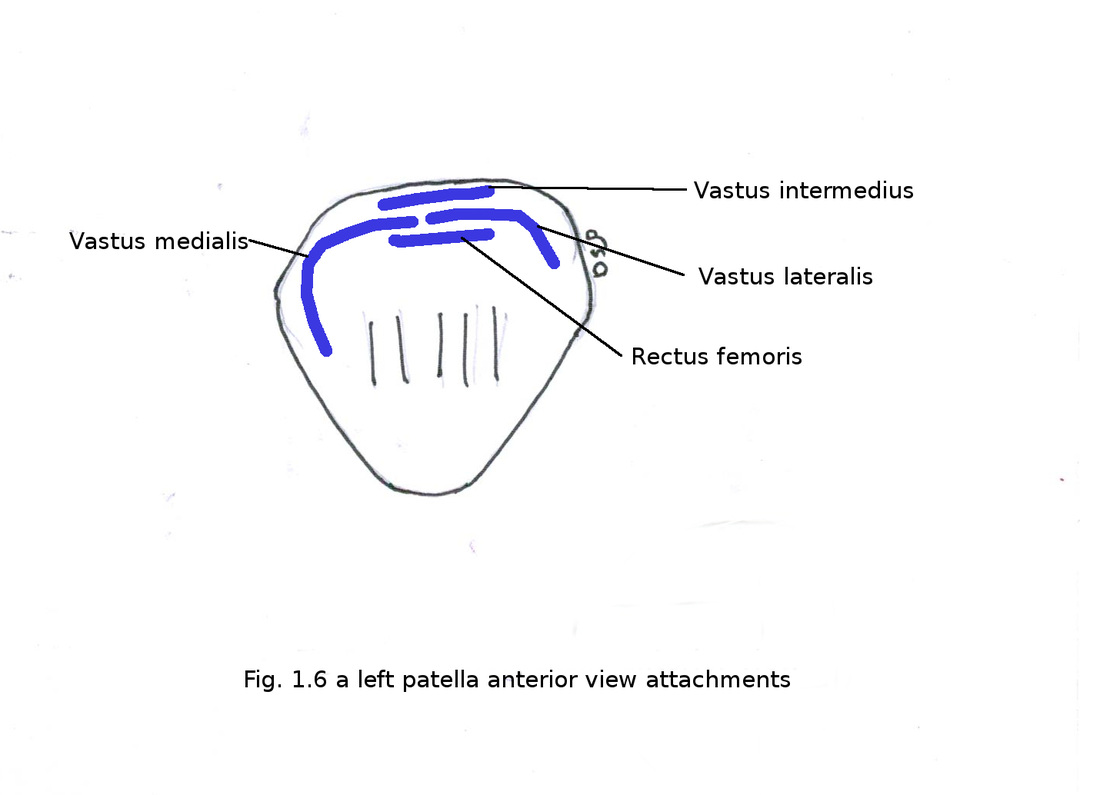
Insertion of Muscles :
Rectus femoris shows insertion on base of patella.
Vastus lateralis shows insertion on base of patella on lateral 2/3rd part and on lateral border upper 1/3rd part.
Vastus medialis shows insertion on base of patella on medial 1/3rd part and on medial border upper 2/3rd part.
Vastus intermedius shows insertion on base of patella.
Arrangement of insertion anterior to posterior on base of patella is as follows rectus femoris in first plane, vastus lateralis and vastus medialis in second plane, vastus intermedius in 3rd plane.
Other Attachments :
Patellar retinaculum shows attachment on lower 1/3rd part of medial border and lower 2/3 rd part of lateral border.
Ligamentum patellae shows attachment on apex of patella.
Side determination:
By placing patella with apex downwards it will tilt towards respective side to which it belong. Articular area should be posteriorly. This is because of large articular area present on lateral side.
Ossification:
Patella ossify from numerous centres which appears between 3rd to 6th year. All centres fuse with each other immediately after appearance.
Applied anatomy:
1. Patella may be present in two or three pieces.
2. There is tendency of patella to dislocate laterally this is prevented by attachment of vastus medialis more on medial border of patella.
3. Runners knee: pain in relation to patella due to damage to articular cartilage of patella. It is common in persons who runs more.
It is large and big sesamoid bone which ossifies in the tendon of quadriceps femoris muscle.
It is a triangular bone.
It shows an apex, base (upper border), medial and lateral borders and two surface anterior and posterior.
Apex is pointed lower end of patella. Base is upper margin of patella. Medial and lateral borders goes downward towards apex.
Anterior surface is covered skin only so it is subcutaneous. A pre-patellar bursa present in relation with it. Vertical lines present on this surface. Posterior surface is articular for articulation with lower end of femur but near apex it is nonarticular. It is divided by vertical prominent elevation (ridge) into lateral and medial parts which are large and small respectively. Medial part again divided by a vertical ridge into a small medial segment and large lateral segment. Both large lateral segment (medial part) and lateral part are subdivided by two transverse lines into upper, middle, and lower areas.
Areas which comes in contact with patellar articular area of femur in different positions :
upper area - during mild flexion
middle area - during semiflexion
lower area – during mild extension
medial area – during full flexion
During full extension patella floats anterior to knee joint.
Insertion of Muscles :
Rectus femoris shows insertion on base of patella.
Vastus lateralis shows insertion on base of patella on lateral 2/3rd part and on lateral border upper 1/3rd part.
Vastus medialis shows insertion on base of patella on medial 1/3rd part and on medial border upper 2/3rd part.
Vastus intermedius shows insertion on base of patella.
Arrangement of insertion anterior to posterior on base of patella is as follows rectus femoris in first plane, vastus lateralis and vastus medialis in second plane, vastus intermedius in 3rd plane.
Other Attachments :
Patellar retinaculum shows attachment on lower 1/3rd part of medial border and lower 2/3 rd part of lateral border.
Ligamentum patellae shows attachment on apex of patella.
Side determination:
By placing patella with apex downwards it will tilt towards respective side to which it belong. Articular area should be posteriorly. This is because of large articular area present on lateral side.
Ossification:
Patella ossify from numerous centres which appears between 3rd to 6th year. All centres fuse with each other immediately after appearance.
Applied anatomy:
1. Patella may be present in two or three pieces.
2. There is tendency of patella to dislocate laterally this is prevented by attachment of vastus medialis more on medial border of patella.
3. Runners knee: pain in relation to patella due to damage to articular cartilage of patella. It is common in persons who runs more.
FIBULA
Fibula present on lateral aspect of tibia.
Parts of fibula:
Upper end
Shaft
Lower end
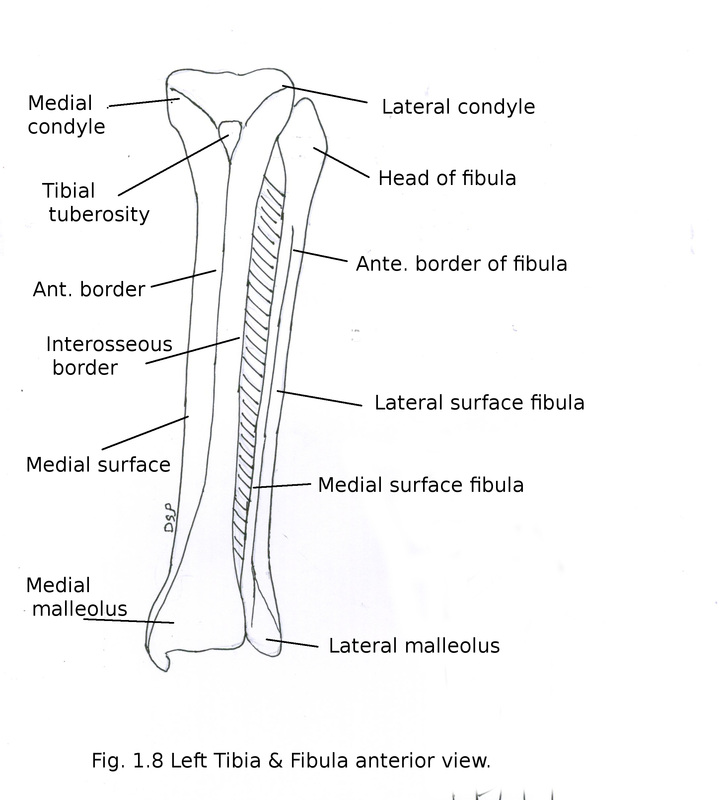
Upper end
It shows head and neck. Head shows an articular facet for articulation with lateral condyle of tibia, styloid process. Neck of fibula is constricted part below head.
Shaft
It shows three borders anterior, posterior and interosseous. Three surfaces medial, lateral and posterior. Anterior border goes downwards and in lower part it divides forming a triangular area on lateral aspect of lateral malleolus. Posterior border continue downwards as posterior border of lateral malleolus. Interosseous border is a medial border.
Medial surface is between anterior and interosseous border. It is very narrow in proximal part. Lateral surface is area between anterior and posterior borders. Posterior surface is between interosseous and posterior border. It shows a medial crest in proximal 2/3rd part a border like line. This crest divide posterior surface into anterior and posterior parts. Anterior part is concave and posterior part is flat.
Lower end
It shows lateral malleolus. Lateral malleolus shows three surfaces lateral, medial and posterior. An anterior border is present which is continuation of anterior division of anterior border of shaft. Lateral surface formed by division of anterior border of shaft. Medial surface shows an triangular articular area for articulation with talus and posterior part of it shows malleolar fossa (this will help in identification of side of fibula). Above articular facet there is a rough triangular area. Posterior surface shows a groove.
Fibula present on lateral aspect of tibia.
Parts of fibula:
Upper end
Shaft
Lower end
Upper end
It shows head and neck. Head shows an articular facet for articulation with lateral condyle of tibia, styloid process. Neck of fibula is constricted part below head.
Shaft
It shows three borders anterior, posterior and interosseous. Three surfaces medial, lateral and posterior. Anterior border goes downwards and in lower part it divides forming a triangular area on lateral aspect of lateral malleolus. Posterior border continue downwards as posterior border of lateral malleolus. Interosseous border is a medial border.
Medial surface is between anterior and interosseous border. It is very narrow in proximal part. Lateral surface is area between anterior and posterior borders. Posterior surface is between interosseous and posterior border. It shows a medial crest in proximal 2/3rd part a border like line. This crest divide posterior surface into anterior and posterior parts. Anterior part is concave and posterior part is flat.
Lower end
It shows lateral malleolus. Lateral malleolus shows three surfaces lateral, medial and posterior. An anterior border is present which is continuation of anterior division of anterior border of shaft. Lateral surface formed by division of anterior border of shaft. Medial surface shows an triangular articular area for articulation with talus and posterior part of it shows malleolar fossa (this will help in identification of side of fibula). Above articular facet there is a rough triangular area. Posterior surface shows a groove.
Attachments
Origin of muscles:
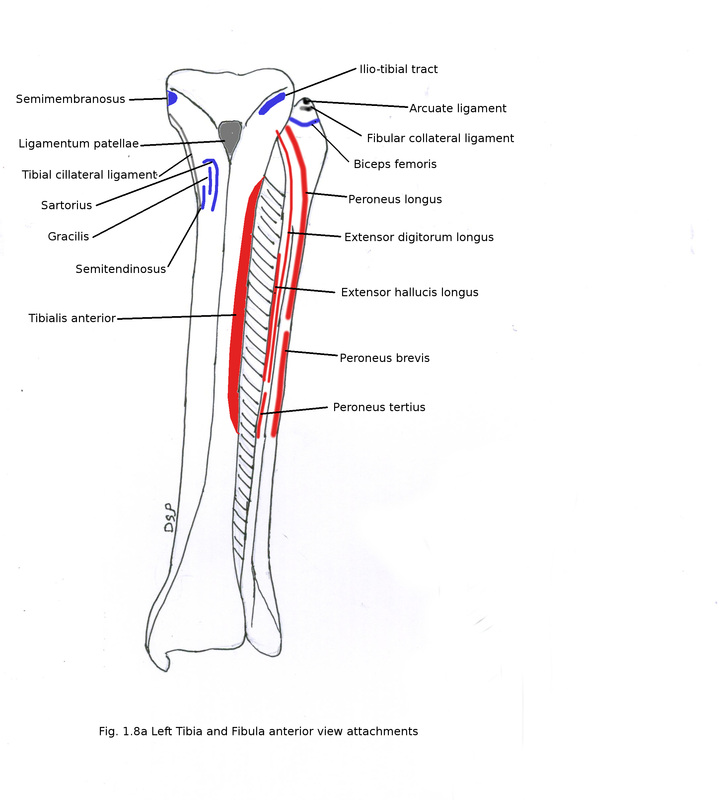
Extensor digitorum longus shows origin from upper 3/4th part of medial surface of shaft.
Extensor hallucis longus shows origin from middle 2/4th part of medial surface of shaft medial to origin of extensor digitorum longus.
Peroneus tertius shows origin from lower 1/4th part of medial surface of shaft.
Peroneus longus and brevis shows origin from upper 2/3rd and middle 2/3rd part of lateral surface of shaft.
Tibialis posterior shows origin from anterior part of posterior surface formed by medial crest of shaft upper 3/4th part.
Soleus shows origin from posterior part of posterior surface formed by medial crest of shaft in upper 1/4th part.
Flexor hallucis longus shows origin from posterior part of posterior surface formed by medial crest of shaft in lower 3/4th part.
Insertion of Muscles:
Biceps femoris shows insertion on head.
Other Attachments :
Fibular collateral ligament shows attachment in front of styloid process between attachment of biceps femoris.
Capsule of knee joint shows attachment on margin of articular facet of head.
Anterior intermuscular septum shows attachment on anterior border of shaft.
Posterior intermuscular septum shows attachment on posterior border of shaft.
Superior extensor retinaculum shows attachment on anterior margin of lower triangular area of lateral malleolus.
Superior peroneal retinaculum shows attachment on posterior margin of lower triangular area.
Interosseous membrane shows attachment on medial border of shaft.
Inferior transverse tibio-fibular ligament shows attachment on malleolar fossa.
Posterior talo-fibular ligament shows attachment on malleolar fossa.
Anterior talo-fibular ligament shows attachment on anterior border of lateral malleolus.
Calcaneo-fibular ligament shows attachment on a notch anterior margin of lateral malleolus.
Interosseous tibio-fibular ligament shows attachment on triangular rough surface above facet for talus.
Anterior and posterior tibio-fibular ligament shows attachment on triangular rough surface above facet for talus anteriorly and posteriorly respectively.
Ossification:
1 primary centre for shaft and 2 secondary centres for upper and lower end. Primary centre appears in 8th week of intrauterine life. Secondary centres one for lower end appears in 1st to 2nd year; second for upper end appears in 3rd to 4th year. Fusion with shaft of lower end takes place between 15th to 17th year and upper end between in 17th to 19th year.
Centre which appears fuses first so it violates law of ossification. Reason for this is centre of ossification for pressure epiphysis appears early as compared to traction epiphysis. Upper end of fibula is traction epiphysis and lower end is pressure epiphysis.
Applied anatomy:
1. Fibula used as spare bone for bone grafting.
Origin of muscles:
Extensor digitorum longus shows origin from upper 3/4th part of medial surface of shaft.
Extensor hallucis longus shows origin from middle 2/4th part of medial surface of shaft medial to origin of extensor digitorum longus.
Peroneus tertius shows origin from lower 1/4th part of medial surface of shaft.
Peroneus longus and brevis shows origin from upper 2/3rd and middle 2/3rd part of lateral surface of shaft.
Tibialis posterior shows origin from anterior part of posterior surface formed by medial crest of shaft upper 3/4th part.
Soleus shows origin from posterior part of posterior surface formed by medial crest of shaft in upper 1/4th part.
Flexor hallucis longus shows origin from posterior part of posterior surface formed by medial crest of shaft in lower 3/4th part.
Insertion of Muscles:
Biceps femoris shows insertion on head.
Other Attachments :
Fibular collateral ligament shows attachment in front of styloid process between attachment of biceps femoris.
Capsule of knee joint shows attachment on margin of articular facet of head.
Anterior intermuscular septum shows attachment on anterior border of shaft.
Posterior intermuscular septum shows attachment on posterior border of shaft.
Superior extensor retinaculum shows attachment on anterior margin of lower triangular area of lateral malleolus.
Superior peroneal retinaculum shows attachment on posterior margin of lower triangular area.
Interosseous membrane shows attachment on medial border of shaft.
Inferior transverse tibio-fibular ligament shows attachment on malleolar fossa.
Posterior talo-fibular ligament shows attachment on malleolar fossa.
Anterior talo-fibular ligament shows attachment on anterior border of lateral malleolus.
Calcaneo-fibular ligament shows attachment on a notch anterior margin of lateral malleolus.
Interosseous tibio-fibular ligament shows attachment on triangular rough surface above facet for talus.
Anterior and posterior tibio-fibular ligament shows attachment on triangular rough surface above facet for talus anteriorly and posteriorly respectively.
Ossification:
1 primary centre for shaft and 2 secondary centres for upper and lower end. Primary centre appears in 8th week of intrauterine life. Secondary centres one for lower end appears in 1st to 2nd year; second for upper end appears in 3rd to 4th year. Fusion with shaft of lower end takes place between 15th to 17th year and upper end between in 17th to 19th year.
Centre which appears fuses first so it violates law of ossification. Reason for this is centre of ossification for pressure epiphysis appears early as compared to traction epiphysis. Upper end of fibula is traction epiphysis and lower end is pressure epiphysis.
Applied anatomy:
1. Fibula used as spare bone for bone grafting.
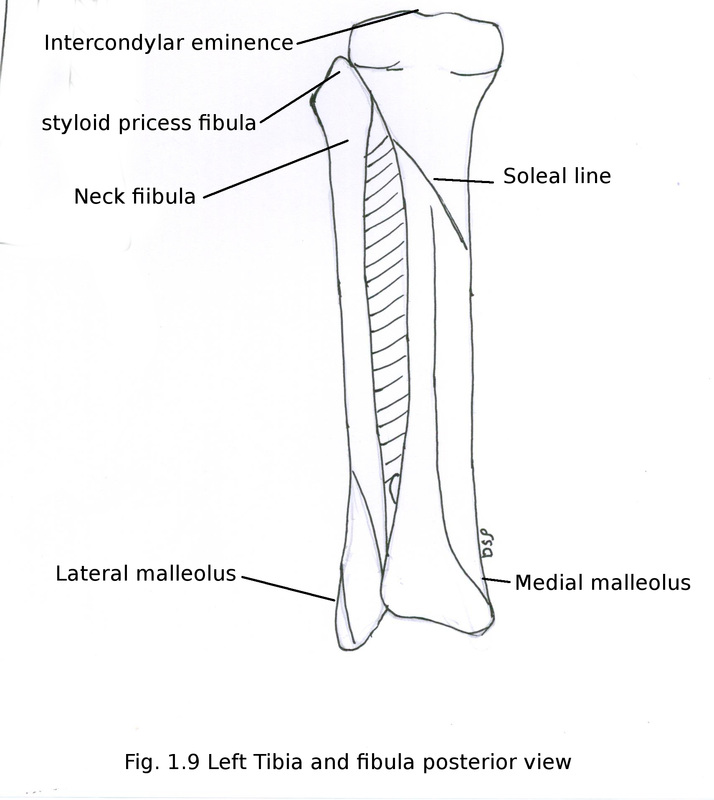
TIBIA
Tibia present on medial aspect of leg medial to fibula.
Parts of tibia:
Upper end
Shaft
Lower end
Upper end
It shows expanded two condyles medial and lateral. Superior surface of condyles shows articular areas. In between these two articular areas of condyles inter-condylar area present. Inter-condylar eminence present in the middle of this area. An facet for articulation with head of fibula present on postero-inferior aspect of lateral condyle. Lateral condyle shows a groove for tendon of popliteus muscle on posterior aspect. An triagular area present on anterior aspect of condyles apex of which formed by tibial tuberosity. Tibial tuberosity is a projection present on upper end of tibia anteriorly. It is rough distally and smooth proximally.
Shaft
It is triangular on section. It is shows three borders anterior, medial and lateral and three surfaces medial, lateral and posterior. Anterior border goes downwards from tibial tuberosity to medial malleolus forming anterior margin and slightly curved below. It is subcutaneous. Medial border starts from medial aspect of medial condyle and in lower part it forms posterior border of medial malleolus. Lateral border or interosseous border continue downwards from lateral condyle anterior to facet for fibula below forms triangular rough area.
Medial surface is between anterior and medial border. It is large and subcutaneous in its entire extend. Lateral surface is area between anterior and lateral borders. Posterior surface is between lateral and medial borders. It shows a soleal line in upper part of this surface. Soleal line goes downwards and medially.
Lower end
It shows an articular facet for fibula laterally. It shows four surfaces lateral, medial, anterior, posterior and inferior. Inferior surface is articular for articulation with talus.
It shows an extension downwards named medial malleolus. Medial malleolus shows four surfaces lateral, medial, anterior and posterior. Medial surface covered only by skin so subcutaneous. Lateral surface shows an articular facet for talus. Posterior surface shows a groove for tendon of tibialis posterior.
Tibia present on medial aspect of leg medial to fibula.
Parts of tibia:
Upper end
Shaft
Lower end
Upper end
It shows expanded two condyles medial and lateral. Superior surface of condyles shows articular areas. In between these two articular areas of condyles inter-condylar area present. Inter-condylar eminence present in the middle of this area. An facet for articulation with head of fibula present on postero-inferior aspect of lateral condyle. Lateral condyle shows a groove for tendon of popliteus muscle on posterior aspect. An triagular area present on anterior aspect of condyles apex of which formed by tibial tuberosity. Tibial tuberosity is a projection present on upper end of tibia anteriorly. It is rough distally and smooth proximally.
Shaft
It is triangular on section. It is shows three borders anterior, medial and lateral and three surfaces medial, lateral and posterior. Anterior border goes downwards from tibial tuberosity to medial malleolus forming anterior margin and slightly curved below. It is subcutaneous. Medial border starts from medial aspect of medial condyle and in lower part it forms posterior border of medial malleolus. Lateral border or interosseous border continue downwards from lateral condyle anterior to facet for fibula below forms triangular rough area.
Medial surface is between anterior and medial border. It is large and subcutaneous in its entire extend. Lateral surface is area between anterior and lateral borders. Posterior surface is between lateral and medial borders. It shows a soleal line in upper part of this surface. Soleal line goes downwards and medially.
Lower end
It shows an articular facet for fibula laterally. It shows four surfaces lateral, medial, anterior, posterior and inferior. Inferior surface is articular for articulation with talus.
It shows an extension downwards named medial malleolus. Medial malleolus shows four surfaces lateral, medial, anterior and posterior. Medial surface covered only by skin so subcutaneous. Lateral surface shows an articular facet for talus. Posterior surface shows a groove for tendon of tibialis posterior.
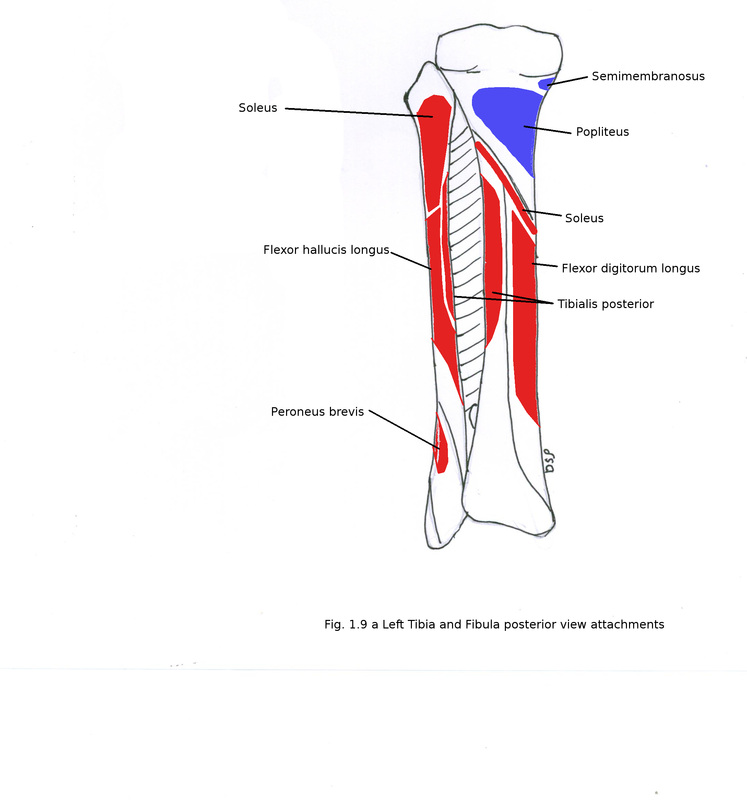
Attachments
Origin of muscles:
Tibialis anterior shows origin from lateral surface of shaft from upper 2/3rd part.
Flexor digitorum longus shows origin from medial part of shaft below soleal line.
Tibialis posterior shows origin from lateral part of shaft below soleal line.
Soleus shows origin from posterior surface of shaft soleal line.
Insertion of Muscles:
Semimembranosus shows insertion on posterior surface of medial condyle.
Sartorius hockey stick shaped, gracilis and semitendinosus shows insertion on upper part medial surface of shaft.
Popliteus shows insertion on posterior surface triangular area of shaft above soleal line in its upper part.
Other Attachments :
Inter-condylar area shows attachment of following structures (anterior to posterior) anterior horn of medial meniscus, anterior cruciate ligament, anterior horn of lateral meniscus, posterior horn of lateral meniscus, posterior horn of medial meniscus, posterior cruciate ligament. (Remember: Medical College London; London Medical College).
Ilio-tibial tract shows attachment on triagular area of lateral condyle.
Ligamentum patellae shows attachment on tibial tuberosity.
Capsule of knee joint shows attachment on margin of upper articular area of condyles .
Capsule of knee joint is pierced by tendon of popliteus near lateral condyle of tibia.
Anterior border of medial malleolus shows attachment of superior extensor retinaculum.
Anterior border of tibia shows attachment of deep fascia of leg.
Medial border of tibia shows attachment of deep fascia of leg, superficial part of tibial collateral ligament.
Flexor retinaculum shows attachment on medial malleolus.
Interosseous membrane shows attachment on lateral border of shaft.
Interosseous inferior tibio-fibular ligament shows attachment on triangular rough surface below formed by lateral border of shaft.
Capsule of ankle joint shows attachment on margin of articular area of lower end.
Medial and lateral patellar retinaculum shows attachment on medial lateral part of triagular areas in relation to condyles.
Ossification:
1 primary centre for shaft and 2 secondary centres for upper and lower end. Primary centre for shaft appears in 7th week of intrauterine life. Secondary centres one for upper end appears at time of birth; second for lower end appears in 1st or 2nd year after birth. Fusion with shaft of upper end takes place between 16th to 18th year and lower end between in 15th to 17th year.
Applied anatomy:
1. Upper end of tibia is common site for osteomyelitis.
2. Nonunion after fracture of lower 1/3rd is common cause is lower end receives less blood supply.
Origin of muscles:
Tibialis anterior shows origin from lateral surface of shaft from upper 2/3rd part.
Flexor digitorum longus shows origin from medial part of shaft below soleal line.
Tibialis posterior shows origin from lateral part of shaft below soleal line.
Soleus shows origin from posterior surface of shaft soleal line.
Insertion of Muscles:
Semimembranosus shows insertion on posterior surface of medial condyle.
Sartorius hockey stick shaped, gracilis and semitendinosus shows insertion on upper part medial surface of shaft.
Popliteus shows insertion on posterior surface triangular area of shaft above soleal line in its upper part.
Other Attachments :
Inter-condylar area shows attachment of following structures (anterior to posterior) anterior horn of medial meniscus, anterior cruciate ligament, anterior horn of lateral meniscus, posterior horn of lateral meniscus, posterior horn of medial meniscus, posterior cruciate ligament. (Remember: Medical College London; London Medical College).
Ilio-tibial tract shows attachment on triagular area of lateral condyle.
Ligamentum patellae shows attachment on tibial tuberosity.
Capsule of knee joint shows attachment on margin of upper articular area of condyles .
Capsule of knee joint is pierced by tendon of popliteus near lateral condyle of tibia.
Anterior border of medial malleolus shows attachment of superior extensor retinaculum.
Anterior border of tibia shows attachment of deep fascia of leg.
Medial border of tibia shows attachment of deep fascia of leg, superficial part of tibial collateral ligament.
Flexor retinaculum shows attachment on medial malleolus.
Interosseous membrane shows attachment on lateral border of shaft.
Interosseous inferior tibio-fibular ligament shows attachment on triangular rough surface below formed by lateral border of shaft.
Capsule of ankle joint shows attachment on margin of articular area of lower end.
Medial and lateral patellar retinaculum shows attachment on medial lateral part of triagular areas in relation to condyles.
Ossification:
1 primary centre for shaft and 2 secondary centres for upper and lower end. Primary centre for shaft appears in 7th week of intrauterine life. Secondary centres one for upper end appears at time of birth; second for lower end appears in 1st or 2nd year after birth. Fusion with shaft of upper end takes place between 16th to 18th year and lower end between in 15th to 17th year.
Applied anatomy:
1. Upper end of tibia is common site for osteomyelitis.
2. Nonunion after fracture of lower 1/3rd is common cause is lower end receives less blood supply.
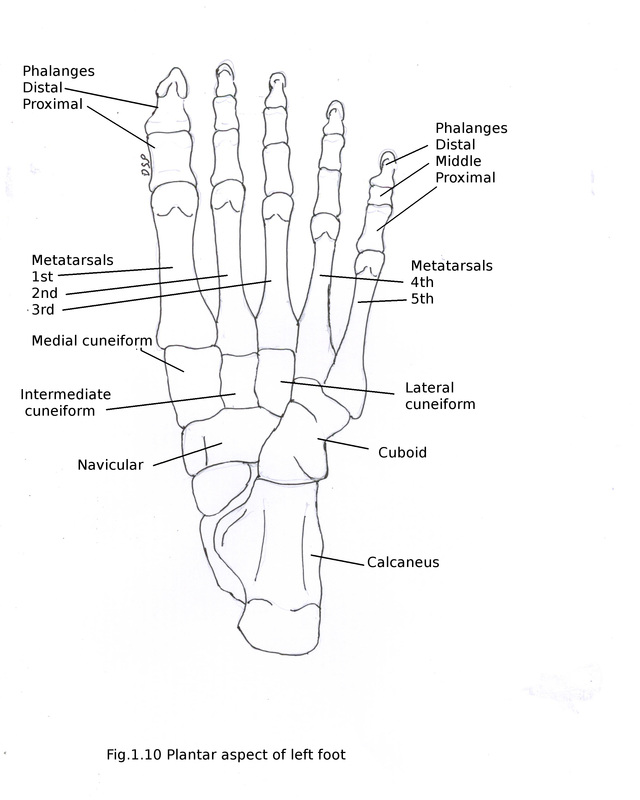
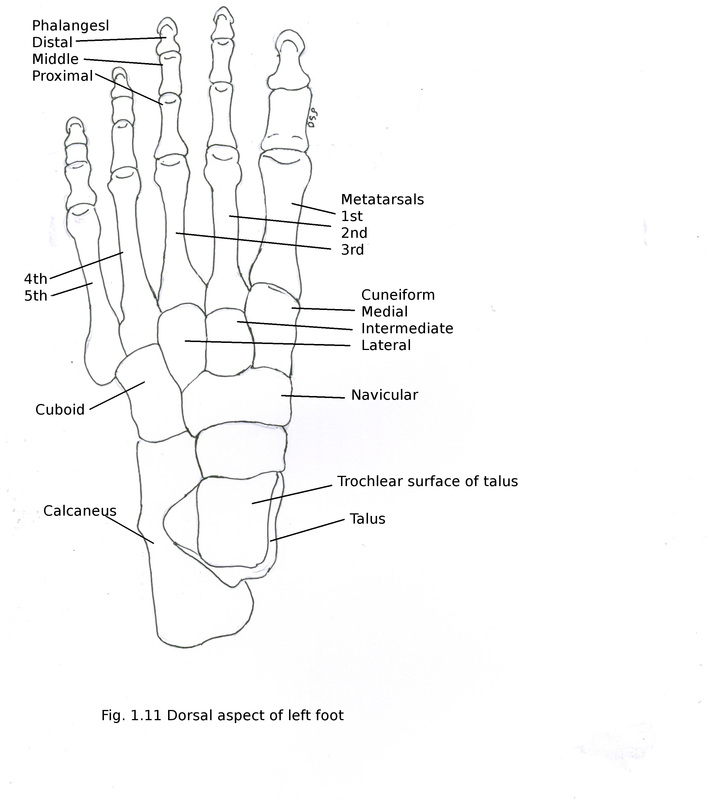
TARSAL BONES
There are 7 tarsal bones in foot.
Proximal row : 1. Talus 2. Calcaneus
Middle row: 1. Navicular
Distal row : 1. Medial cuneiform 2. Intermediate cuneiform 3. Lateral cuneiform 4. Cuboid
Talus
It shows head, neck and body. Head directed anteriorly, downward and forward. It shows convex articular surface. It articulates anteriorly with navicular and inferiorly it shows three articular areas for articulation with upper surface of calcaneus, sustentaculum tali and calcaneo-navicular ligament. Neck directed antero-medially. Sulcus tali a groove present on inferior surface of neck. This groove with a groove on calcaneus forms sinus tarsi. Body antero-posterioly convex and concave side to side on upper aspect. It shows superior, inferior, medial, lateral surfaces. Medial surface having comma shaped articular area. Lateral surface having triangular articular area. These surfaces articulates with lower end of tibia and fibula, medial and lateral malleolus forming ankle joint. Posteriorly there is presence of medial and lateral tubercles forming a groove for tendon of flexor hallucis longus. An articular facet present on inferior surface of body which articulates with middle part of calcaneus.
Calcaneus
It is largest of all tarsal bones. It is directed anteriorly and laterally. It shows anterior, posterior, medial, lateral, superior, inferior (plantar) surfaces. Anterior surface is concavo-convex. It articulates with cuboid. Posterior surface is divided into three parts. These three areas are formed in relation to insertion of tendo-calcaneus. Medial surface is concave from above downward. A projection present on its upper part sustentaculum tali. Lateral surface is flat. It shows two elevations anterior (peroneal trochlea) and posterior. Superior surface shows three area. Anterior 1/3rd is partly rough and partly articular, middle 1/3rd is articular and posterior 1/3rd is rough covered by fibrofatty tissues. It forms sinus tarsi (hollow space) alongwith upper surface of talus. Inferior (plantar) surface shows rough surface and three tubercles two posterior (medial and lateral) and one anterior.
Navicular
It shows two articular surfaces proximal and distal. Proximal concave surface articulates with convex articular surface of head of talus and distal convex articular surface articulates with three cuneiform bones. Distal surface shows shows three vertical triangular facets. Medial surface shows an elevated tuberosity. Superior and inferior surfaces are rough with convex and concave surfaces respectively.
Cuneiform
These are three small wedge shaped bones. Apex of wedge of intermediate and lateral cuneiform are towards plantar surface and medial cuneiform bone towards dorsal surface. Proximally these articulates with triagular facets on navicular bone. Distally articulate with 1st, 2nd and 3rd metatarsal bones with medial, intermediate and lateral cuneiform respectively.
Medial cuneiform
Medial surface of it rough. Lateral surface partly articular along posterior margin articulate with medial surface of intermediate cuneiform and medial surface of 2nd metatarsal near base.
Intermediate cuneiform
Medial surface partly articular along posterior margin articulate with medial cuneiform. Lateral surface partly articular along posterior margin articulate with lateral cuneiform.
Lateral cuneiform
Medial surface partly articular along posterior margin articulate with intermediate cuneiform and lateral surface of 4th metatarsal near base. Lateral surface partly articular along posterior margin articulate with cuboid.
Cuboid
It is cube like in shape. It shows medial, lateral, dorsal, plantar, proximal and distal surfaces. Proximal surface articulate with calcaneus. Distal surface articular shows two articular facets medial quadrilateral and lateral triangular facets. Which articulate with base of 4th and 5th metacarpal bones. Lateral surface is small as compared to medial surface showing a groove. Tendon of peroneus longus runs through this groove. Medial surface articulate with lateral cuneiform and navicular bones. Dorsal surface shows plain area. Plantar surface shows two parts anterior and posterior formed by an oblique ridge and groove.
There are 7 tarsal bones in foot.
Proximal row : 1. Talus 2. Calcaneus
Middle row: 1. Navicular
Distal row : 1. Medial cuneiform 2. Intermediate cuneiform 3. Lateral cuneiform 4. Cuboid
Talus
It shows head, neck and body. Head directed anteriorly, downward and forward. It shows convex articular surface. It articulates anteriorly with navicular and inferiorly it shows three articular areas for articulation with upper surface of calcaneus, sustentaculum tali and calcaneo-navicular ligament. Neck directed antero-medially. Sulcus tali a groove present on inferior surface of neck. This groove with a groove on calcaneus forms sinus tarsi. Body antero-posterioly convex and concave side to side on upper aspect. It shows superior, inferior, medial, lateral surfaces. Medial surface having comma shaped articular area. Lateral surface having triangular articular area. These surfaces articulates with lower end of tibia and fibula, medial and lateral malleolus forming ankle joint. Posteriorly there is presence of medial and lateral tubercles forming a groove for tendon of flexor hallucis longus. An articular facet present on inferior surface of body which articulates with middle part of calcaneus.
Calcaneus
It is largest of all tarsal bones. It is directed anteriorly and laterally. It shows anterior, posterior, medial, lateral, superior, inferior (plantar) surfaces. Anterior surface is concavo-convex. It articulates with cuboid. Posterior surface is divided into three parts. These three areas are formed in relation to insertion of tendo-calcaneus. Medial surface is concave from above downward. A projection present on its upper part sustentaculum tali. Lateral surface is flat. It shows two elevations anterior (peroneal trochlea) and posterior. Superior surface shows three area. Anterior 1/3rd is partly rough and partly articular, middle 1/3rd is articular and posterior 1/3rd is rough covered by fibrofatty tissues. It forms sinus tarsi (hollow space) alongwith upper surface of talus. Inferior (plantar) surface shows rough surface and three tubercles two posterior (medial and lateral) and one anterior.
Navicular
It shows two articular surfaces proximal and distal. Proximal concave surface articulates with convex articular surface of head of talus and distal convex articular surface articulates with three cuneiform bones. Distal surface shows shows three vertical triangular facets. Medial surface shows an elevated tuberosity. Superior and inferior surfaces are rough with convex and concave surfaces respectively.
Cuneiform
These are three small wedge shaped bones. Apex of wedge of intermediate and lateral cuneiform are towards plantar surface and medial cuneiform bone towards dorsal surface. Proximally these articulates with triagular facets on navicular bone. Distally articulate with 1st, 2nd and 3rd metatarsal bones with medial, intermediate and lateral cuneiform respectively.
Medial cuneiform
Medial surface of it rough. Lateral surface partly articular along posterior margin articulate with medial surface of intermediate cuneiform and medial surface of 2nd metatarsal near base.
Intermediate cuneiform
Medial surface partly articular along posterior margin articulate with medial cuneiform. Lateral surface partly articular along posterior margin articulate with lateral cuneiform.
Lateral cuneiform
Medial surface partly articular along posterior margin articulate with intermediate cuneiform and lateral surface of 4th metatarsal near base. Lateral surface partly articular along posterior margin articulate with cuboid.
Cuboid
It is cube like in shape. It shows medial, lateral, dorsal, plantar, proximal and distal surfaces. Proximal surface articulate with calcaneus. Distal surface articular shows two articular facets medial quadrilateral and lateral triangular facets. Which articulate with base of 4th and 5th metacarpal bones. Lateral surface is small as compared to medial surface showing a groove. Tendon of peroneus longus runs through this groove. Medial surface articulate with lateral cuneiform and navicular bones. Dorsal surface shows plain area. Plantar surface shows two parts anterior and posterior formed by an oblique ridge and groove.
Attachments
Origin of muscles:
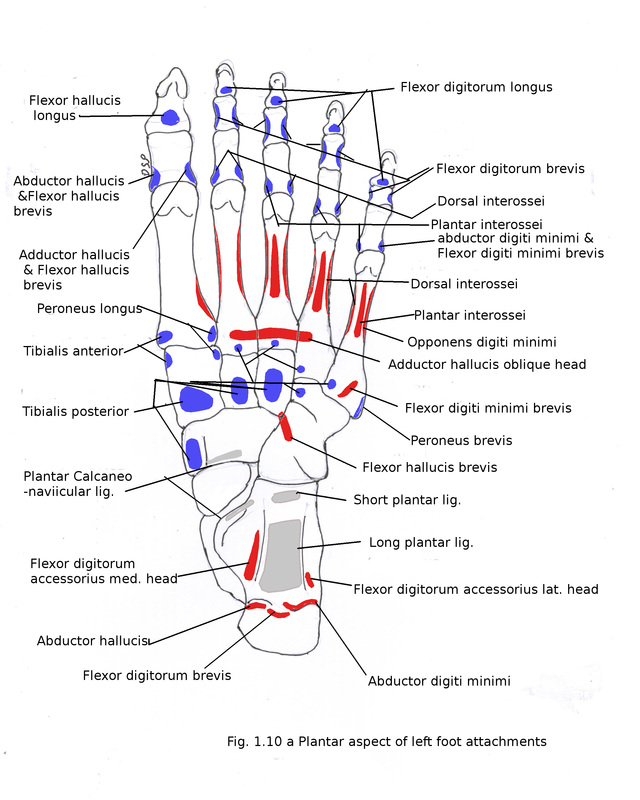
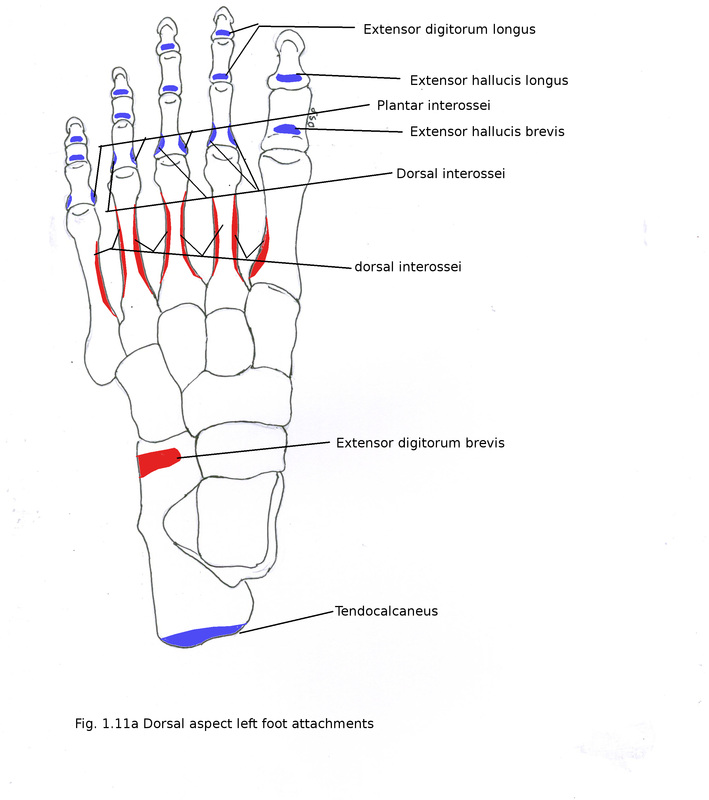
Extensor digitorum brevis shows origin from dorsal surface of anterior part of calcaneus.
Abductor hallucis shows origin from medial tubercle on plantar aspect of calcaneus.
Abductor digiti minimi shows origin from lateral tubercle on plantar aspect of calcaneus.
Flexor hallucis brevis shows origin from plantar aspect of cuboid.
Insertion of Muscles:
Tendo-calcaneus and tendon of plantaris muscle shows insertion on middle part of posterior surface of calcaneus.
Extensor digitorum brevis shows insertion on upper surface of calcaneus on its anterior 1/3rd part.
Flexor digitorum brevis shows origin from medial tubercle on plantar aspect of calcaneus.
Tibialis posterior shows insertion on tuberosity on medial aspect of navicular bone and slips to plantar aspect of medial, intermediate and lateral cuneiform.
Tibialis anterior shows insertion on base of 1st metatarsal and medial aspect of medial cuneiform.
Other Attachments :
Interosseous talo-calcanean ligament shows attachment on inferior surface of neck of talus and upper surfaces of calcaneus forming sinus tarsi.
Bifurcate ligament stem shows attachment on upper surface of calcaneus on its anterior 1/3rd part and Calcaneo-navicular part shows attachment on lateral surface of navicular.
Long plantar ligament shows attachment on triagular area between three tubercles of plantar surface of calcaneus and on oblique ridge of plantar surface of cuboid.
Short plantar ligament shows attachment in front of anterior tubercle on plantar aspect of calcaneus and on posterior part of plantar surface of cuboid.
Inferior extensor retinaculum stem shows attachment on upper surface of calcaneus on its anterior 1/3rd part.
Medial talo-calcanean ligament, Spring ligament, Deltoid ligament shows attachment on sustentaculum tali.
Calcaneo-fibular ligament shows attachment on posterior tubercle present on lateral surface of calcaneus.
Inferior peroneal retinaculum shows attachment on posterior tubercle present on lateral surface of calcaneus.
Plantar calcaneo-navicular (spring) ligament shows attachment on plantar surface of navicular and on sustentaculum tali.
Flexor retinaculum shows attachment on medial tubercle on plantar aspect of calcaneus.
Plantar aponeurosis shows attachment anteriorly on medial tubercle on plantar aspect of calcaneus.
Talonavicular, cuneonavicular, cubonavicular ligament shows attachment on dorsal aspect of navicular.
Ossification:
Primary centre for talus appears in 6th month of intrauterine life. It shows a secondary centre for posterior process which appears during 9-10 years after birth.
For calcaneus two primary centre appears 1st in 3rd month of intrauterine life and 2nd in 6 to 8 years after birth. It fuse with calcaneus during 14 to 16 years.
Navicular primary centre appears during 2 to 3 years after birth.
Cuboid primary centre appears during 8 to 9 month of intrauterine life.
Medial cuneiform primary centre appears during 2 to 3 years after birth.
Intermediate cuneiform primary centre appears during 2 to 3 years after birth.
Lateral cuneiform primary centre appears in 1st year after birth.
Applied anatomy:
1. Fracture of neck of talus may occur due to forceful dorsiflexion at ankle joint. Vessels of talus may goes backward towards body from neck and may cause avascular necrosis of body of talus.
2. Fracture of calcaneus may occur due to fall from height.
3. Navicular may be bipartite (divided into two) when it develops from two separate ossific centres.
Origin of muscles:
Extensor digitorum brevis shows origin from dorsal surface of anterior part of calcaneus.
Abductor hallucis shows origin from medial tubercle on plantar aspect of calcaneus.
Abductor digiti minimi shows origin from lateral tubercle on plantar aspect of calcaneus.
Flexor hallucis brevis shows origin from plantar aspect of cuboid.
Insertion of Muscles:
Tendo-calcaneus and tendon of plantaris muscle shows insertion on middle part of posterior surface of calcaneus.
Extensor digitorum brevis shows insertion on upper surface of calcaneus on its anterior 1/3rd part.
Flexor digitorum brevis shows origin from medial tubercle on plantar aspect of calcaneus.
Tibialis posterior shows insertion on tuberosity on medial aspect of navicular bone and slips to plantar aspect of medial, intermediate and lateral cuneiform.
Tibialis anterior shows insertion on base of 1st metatarsal and medial aspect of medial cuneiform.
Other Attachments :
Interosseous talo-calcanean ligament shows attachment on inferior surface of neck of talus and upper surfaces of calcaneus forming sinus tarsi.
Bifurcate ligament stem shows attachment on upper surface of calcaneus on its anterior 1/3rd part and Calcaneo-navicular part shows attachment on lateral surface of navicular.
Long plantar ligament shows attachment on triagular area between three tubercles of plantar surface of calcaneus and on oblique ridge of plantar surface of cuboid.
Short plantar ligament shows attachment in front of anterior tubercle on plantar aspect of calcaneus and on posterior part of plantar surface of cuboid.
Inferior extensor retinaculum stem shows attachment on upper surface of calcaneus on its anterior 1/3rd part.
Medial talo-calcanean ligament, Spring ligament, Deltoid ligament shows attachment on sustentaculum tali.
Calcaneo-fibular ligament shows attachment on posterior tubercle present on lateral surface of calcaneus.
Inferior peroneal retinaculum shows attachment on posterior tubercle present on lateral surface of calcaneus.
Plantar calcaneo-navicular (spring) ligament shows attachment on plantar surface of navicular and on sustentaculum tali.
Flexor retinaculum shows attachment on medial tubercle on plantar aspect of calcaneus.
Plantar aponeurosis shows attachment anteriorly on medial tubercle on plantar aspect of calcaneus.
Talonavicular, cuneonavicular, cubonavicular ligament shows attachment on dorsal aspect of navicular.
Ossification:
Primary centre for talus appears in 6th month of intrauterine life. It shows a secondary centre for posterior process which appears during 9-10 years after birth.
For calcaneus two primary centre appears 1st in 3rd month of intrauterine life and 2nd in 6 to 8 years after birth. It fuse with calcaneus during 14 to 16 years.
Navicular primary centre appears during 2 to 3 years after birth.
Cuboid primary centre appears during 8 to 9 month of intrauterine life.
Medial cuneiform primary centre appears during 2 to 3 years after birth.
Intermediate cuneiform primary centre appears during 2 to 3 years after birth.
Lateral cuneiform primary centre appears in 1st year after birth.
Applied anatomy:
1. Fracture of neck of talus may occur due to forceful dorsiflexion at ankle joint. Vessels of talus may goes backward towards body from neck and may cause avascular necrosis of body of talus.
2. Fracture of calcaneus may occur due to fall from height.
3. Navicular may be bipartite (divided into two) when it develops from two separate ossific centres.
Metatarsal bones
These are 5 bones of foot numbered from medial to lateral side. Parts head, shaft, base. Head is articular articulating with base of proximal phalanx. Near sides head shows flat part. Shaft shows concave plantar surface and convex dorsal surface. Shaft becomes narrow from base to head. Base of metatarsal articulate with distal row of tarsal bones and other tarsal bones near to it.
Other characters of metatarsal bones.
1st metatarsal
It is a short and thick metatarsal bone. Its base is concave for articulation with medial cuneiform.
2nd metatarsal
It is a longest metatarsal bone. Its base shows four articular facets one proximal for intermediate cuneiform, two laterally for 3rd metatarsal base and lateral cuneiform and one medially for medial cuneiform.
3rd metatarsal
It shows a triangular base for articulation with lateral cuneiform. Medially shows two facets for 2nd metatarsal and laterally a single facet for 4th metatarsal.
4th metatarsal
A single quadrilateral facet present on proximal part of its base for cuboid. Laterally a single facet for 5th metatarsal. Medially a facet for 3rd metatarsal.
5th metatarsal
It shows a tuberosity near base laterally. Proximally a base articulate with cuboid. Medially articulate with 4th metatarsal.
Origin of muscles, Insertion of Muscles, Other Attachments:
1st metatarsal
Tibialis anterior shows insertion on base medial side of 1st metatarsal.
Peroneus longus shows insertion on inferolateral side of 1st metatarsal.
Lateral area of shaft shows origin of medial head of 1st dorsal interosseous.
2nd metatarsal
Medial and lateral area of the shaft shows origin of lateral head of 1st and medial head of 2nd dorsal interosseous.
Adductor hallucis oblique head shows origin from base of second metatarsal on plantar aspect.
3rd metatarsal
Medial and lateral surface of shaft shows origin of lateral head of second dorsal interosseous and medial head of third dorsal interosseous muscles respectively.
Medial surface on plantar surface of shaft shows origin of 1st plantar interosseous.
Oblique head of adductor hallucis shows origin from transverse line on plantar surface of base on plantar surface.
4th metatarsal
Medial and lateral surfaces of shaft shows origin of lateral head of 3rd dorsal interosseous and medial head of 4th dorsal interosseous respectively.
Medial area plantar surface of shaft shows origin of the 2nd plantar interosseous muscle.
Oblique head of adductor hallucis shows origin from transverse line on plantar surface of base on plantar surface.
5th metatarsal
Medial surface of shaft shows origin of lateral head of 4th dorsal interosseous.
Medial surface of plantar surface of shaft shows origin of 3rd plantar interosseous muscles.
Peroneus tertius shows insertion on dorsal surface near base.
Peroneus brevis shows insertion on tuberosity.
Plantar surface near base shows origin of flexor digiti minimi.
Ossification:
One primary centre for shaft and one secondary centres for the head of 2nd to 5th metatarsal and base of first metatarsal. Primary centre appears in 8th week of intrauterine life and Secondary centre appear during second year and fuses with shaft after 17 to 20 year.
Applied anatomy:
March fracture : It occurs in soldiers in 2nd, 3rd, 4th and 5th metatarsal bones due to sudden continuous stress after long rest.
These are 5 bones of foot numbered from medial to lateral side. Parts head, shaft, base. Head is articular articulating with base of proximal phalanx. Near sides head shows flat part. Shaft shows concave plantar surface and convex dorsal surface. Shaft becomes narrow from base to head. Base of metatarsal articulate with distal row of tarsal bones and other tarsal bones near to it.
Other characters of metatarsal bones.
1st metatarsal
It is a short and thick metatarsal bone. Its base is concave for articulation with medial cuneiform.
2nd metatarsal
It is a longest metatarsal bone. Its base shows four articular facets one proximal for intermediate cuneiform, two laterally for 3rd metatarsal base and lateral cuneiform and one medially for medial cuneiform.
3rd metatarsal
It shows a triangular base for articulation with lateral cuneiform. Medially shows two facets for 2nd metatarsal and laterally a single facet for 4th metatarsal.
4th metatarsal
A single quadrilateral facet present on proximal part of its base for cuboid. Laterally a single facet for 5th metatarsal. Medially a facet for 3rd metatarsal.
5th metatarsal
It shows a tuberosity near base laterally. Proximally a base articulate with cuboid. Medially articulate with 4th metatarsal.
Origin of muscles, Insertion of Muscles, Other Attachments:
1st metatarsal
Tibialis anterior shows insertion on base medial side of 1st metatarsal.
Peroneus longus shows insertion on inferolateral side of 1st metatarsal.
Lateral area of shaft shows origin of medial head of 1st dorsal interosseous.
2nd metatarsal
Medial and lateral area of the shaft shows origin of lateral head of 1st and medial head of 2nd dorsal interosseous.
Adductor hallucis oblique head shows origin from base of second metatarsal on plantar aspect.
3rd metatarsal
Medial and lateral surface of shaft shows origin of lateral head of second dorsal interosseous and medial head of third dorsal interosseous muscles respectively.
Medial surface on plantar surface of shaft shows origin of 1st plantar interosseous.
Oblique head of adductor hallucis shows origin from transverse line on plantar surface of base on plantar surface.
4th metatarsal
Medial and lateral surfaces of shaft shows origin of lateral head of 3rd dorsal interosseous and medial head of 4th dorsal interosseous respectively.
Medial area plantar surface of shaft shows origin of the 2nd plantar interosseous muscle.
Oblique head of adductor hallucis shows origin from transverse line on plantar surface of base on plantar surface.
5th metatarsal
Medial surface of shaft shows origin of lateral head of 4th dorsal interosseous.
Medial surface of plantar surface of shaft shows origin of 3rd plantar interosseous muscles.
Peroneus tertius shows insertion on dorsal surface near base.
Peroneus brevis shows insertion on tuberosity.
Plantar surface near base shows origin of flexor digiti minimi.
Ossification:
One primary centre for shaft and one secondary centres for the head of 2nd to 5th metatarsal and base of first metatarsal. Primary centre appears in 8th week of intrauterine life and Secondary centre appear during second year and fuses with shaft after 17 to 20 year.
Applied anatomy:
March fracture : It occurs in soldiers in 2nd, 3rd, 4th and 5th metatarsal bones due to sudden continuous stress after long rest.
PHALANGES
Phalanges are 14 in each foot. 3 for lateral 4 toes and 2 for great toe. Phalanges are proximal, middle and distal but in great toe only proximal and distal phalanx present. Each phalanx shows base, shaft and head.
Base of proximal phalanx is concave for articulation with head of metatarsal bone. Bases of middle and distal phalanges shows broad base. Shaft of phalanx is convex on its dorsal surface. Plantar surface of phalanx is concave. The head of distal phalanx shows rough tuberosity on its plantar aspect.
Attachments:
Distal phalanges of lateral 4 toes show the insertion near base on plantar surface of flexor digitorum longus and on dorsal surface near base insertion of extensor digitorum longus along with tendons of lumbricals and interossei.
Distal phalanx of great toe shows insertion of flexor hallucis longus on plantar surface and extensor hallucis longus on dorsal surface near base.
Middle phalanx of lateral four toes on both side shows insertion of flexor digitorum brevis, dorsal surface near base shows insertion of extensor digitorum longus.
Base of proximal phalanx of 2nd toe shows insertion of 1st dorsal interosseous medially, 2nd dorsal interosseous laterally.
Base of proximal phalanx of 3rd toe shows insertion of 1st plantar interosseous medially, 3rd dorsal interosseous laterally.
Base of proximal phalanx of 4th toe shows insertion of 2nd plantar interosseous medially, 4th dorsal interosseous laterally.
Base of proximal phalanx of 5th toe shows insertion of 3rd plantar interosseous medially, abductor digiti minimi and flexor digiti minimi brevis laterally.
Base of proximal phalanx great toe shows insertion of following structures abductor hallucis, medial tendon of flexor hallucis brevis medially, adductor hallucis and lateral tendon of flexor hallucis brevis laterally. On dorsal surface near base shows insertion of extensor hallucis brevis.
Ossification:
One primary centre for proximal phalanges appear for shaft in 10 to 15 week of intrauterine life. Middle phalanx after proximal phalanx and distal phalanx between 9 or 12 week of intrauterine life.
Secondary centre for base of phalanx appear in second to eight year. All the centre fuse with each other during 16 to 18 years of life.
Phalanges are 14 in each foot. 3 for lateral 4 toes and 2 for great toe. Phalanges are proximal, middle and distal but in great toe only proximal and distal phalanx present. Each phalanx shows base, shaft and head.
Base of proximal phalanx is concave for articulation with head of metatarsal bone. Bases of middle and distal phalanges shows broad base. Shaft of phalanx is convex on its dorsal surface. Plantar surface of phalanx is concave. The head of distal phalanx shows rough tuberosity on its plantar aspect.
Attachments:
Distal phalanges of lateral 4 toes show the insertion near base on plantar surface of flexor digitorum longus and on dorsal surface near base insertion of extensor digitorum longus along with tendons of lumbricals and interossei.
Distal phalanx of great toe shows insertion of flexor hallucis longus on plantar surface and extensor hallucis longus on dorsal surface near base.
Middle phalanx of lateral four toes on both side shows insertion of flexor digitorum brevis, dorsal surface near base shows insertion of extensor digitorum longus.
Base of proximal phalanx of 2nd toe shows insertion of 1st dorsal interosseous medially, 2nd dorsal interosseous laterally.
Base of proximal phalanx of 3rd toe shows insertion of 1st plantar interosseous medially, 3rd dorsal interosseous laterally.
Base of proximal phalanx of 4th toe shows insertion of 2nd plantar interosseous medially, 4th dorsal interosseous laterally.
Base of proximal phalanx of 5th toe shows insertion of 3rd plantar interosseous medially, abductor digiti minimi and flexor digiti minimi brevis laterally.
Base of proximal phalanx great toe shows insertion of following structures abductor hallucis, medial tendon of flexor hallucis brevis medially, adductor hallucis and lateral tendon of flexor hallucis brevis laterally. On dorsal surface near base shows insertion of extensor hallucis brevis.
Ossification:
One primary centre for proximal phalanges appear for shaft in 10 to 15 week of intrauterine life. Middle phalanx after proximal phalanx and distal phalanx between 9 or 12 week of intrauterine life.
Secondary centre for base of phalanx appear in second to eight year. All the centre fuse with each other during 16 to 18 years of life.
