JOINTS OF LOWER LIMB
PELVIC GIRDLE
It transmits weight and protects structures. It consists of two hip bones formed by ilium, ischium, pubis and one sacrum. Having three joints one pubic symphysis anteriorly and two sacroiliac joint posteriorly. No movements takes place at these joints.
HIP JOINT
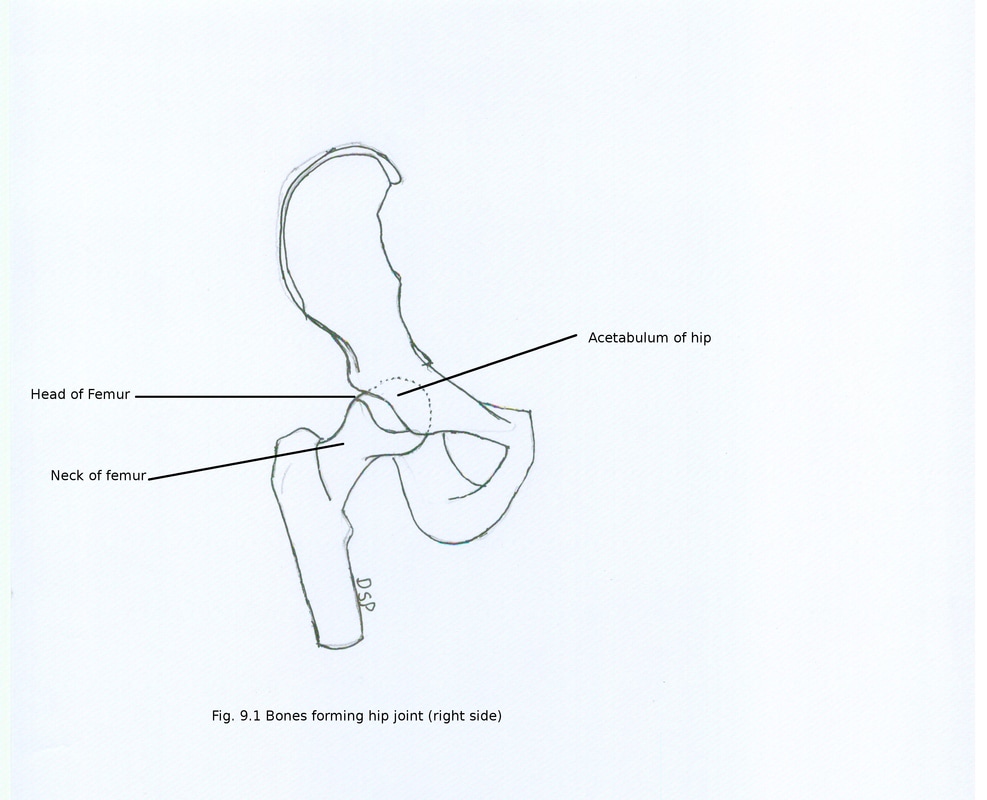
It is a ball and socket type of synovial joint.
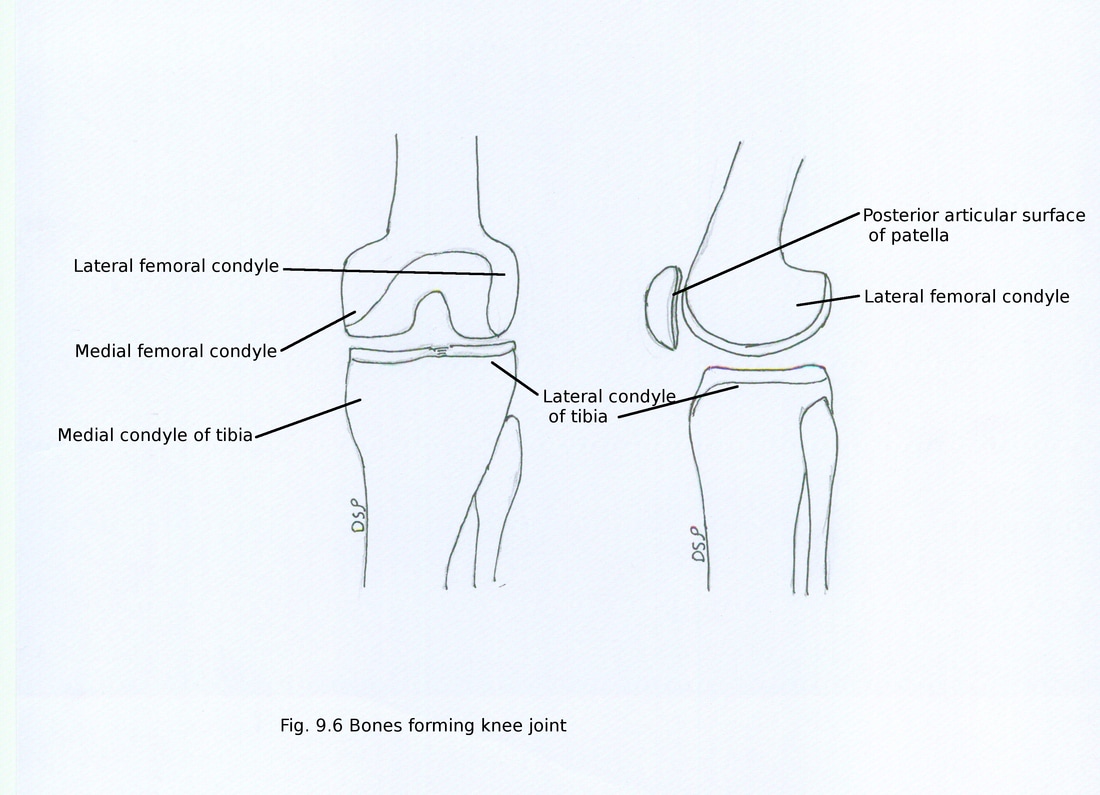
Bones forming joint :
Head of femur and acetabulum of hip bone. Articular surface of head of femur forms more than half of sphere is covered by an articular hyaline cartilage deficient in center for pit or fovea showing attachment of ligamentum teres and acetabulum shows fibro-cartilagenous rim near periphery named acetabular labrum deficient inferiorly near acetabular notch, articular surface lunate and non-articular acetabular fossa containing fat.
PELVIC GIRDLE
It transmits weight and protects structures. It consists of two hip bones formed by ilium, ischium, pubis and one sacrum. Having three joints one pubic symphysis anteriorly and two sacroiliac joint posteriorly. No movements takes place at these joints.
HIP JOINT
It is a ball and socket type of synovial joint.
Bones forming joint :
Head of femur and acetabulum of hip bone. Articular surface of head of femur forms more than half of sphere is covered by an articular hyaline cartilage deficient in center for pit or fovea showing attachment of ligamentum teres and acetabulum shows fibro-cartilagenous rim near periphery named acetabular labrum deficient inferiorly near acetabular notch, articular surface lunate and non-articular acetabular fossa containing fat.
Ligaments :
1.Capsule
2. Acetabular labrum
3. Transverse acetabular ligament
4. Ligamentum teres femoris (ligament of head of femur)
5. Ilio-femoral ligament
6. Pubo-femoral ligament
7. Ischio-femoral ligament
1. Capsule :
Capsule shows attachment medially near margins of acetabulum 5 to 6 mm above labrum and transverse acetabular ligament. Laterally shows attachment anteriorly on intertrochanteric line, posteriorly 1cm medial to intertrochanteric crest, above and below shows attachment on neck of femur close to greater trochanter and in front of lesser trochanter respectively. From intertrochanteric line few fibres of capsule goes medially along the neck forming retinacular fibres. Capsule is thick and strong anterosuperiorly but inferomedially weak. Deep fibres of capsule are circularly arranged while outer fibres are longitudinally arranged. Zona orbicularis are circularly arranged inner fibres of capsule around neck of femur.
Synovial membrane covers inner aspect of capsule, intracapsular part of femoral neck, acetabular labrum, transverse acetabular ligament, ligamentum teres and fat present in acetabular fossa. Synovial membrane may come out through a small gap on anterior aspect of capsule present in between pubo-femoral and ilio-femoral ligament.
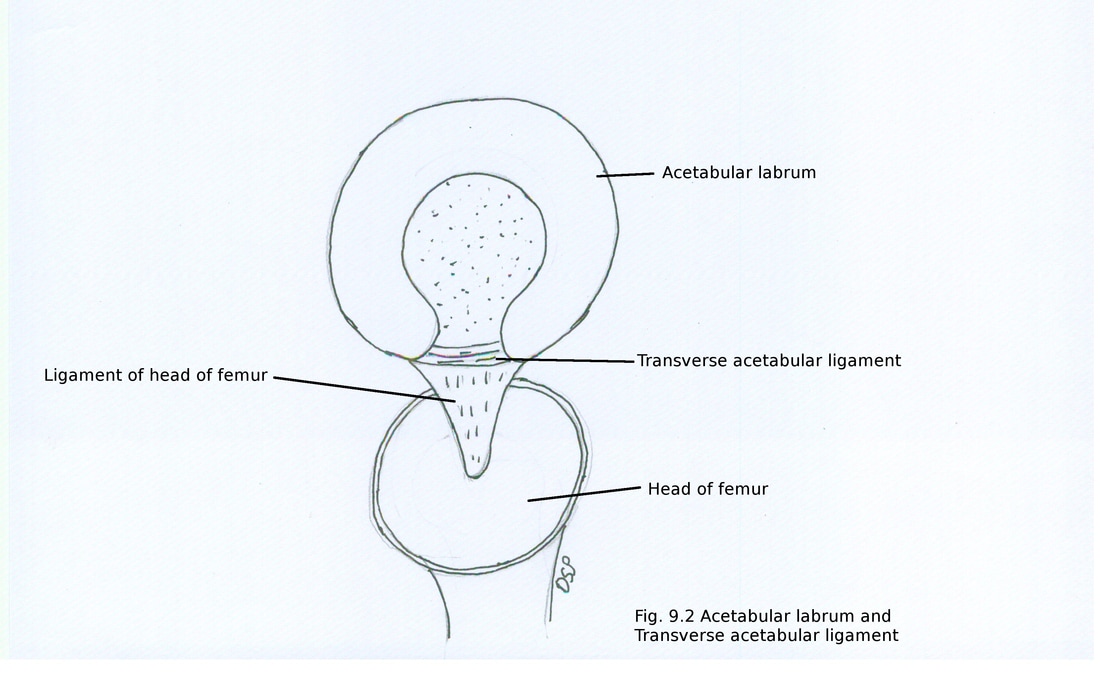
2. Acetabular labrum
It is a cartilaginous rim showing attachment on margin of acetabulum. It is triangular in shape on cross section. Its functions are deepens the acetabular socket and hold head of femur tightly.
3. Transverse acetabular ligament
It is present in relation with acetabular notch bridging the notch. It is a noncartilagenous part of acetabular labrum. It converts acetabular notch into foramen for transmission of acetabular vessels and nerves to hip joint.
4. Ligamentum teres femoris (ligament of head of femur)
It is a triangular, flat and fibrous band. Its apex shows attachment on fovea present on femoral head. Base shows attachment on two margins of acetabular notch and it blends with transverse acetabular ligament. It is covered by synovial membrane. It become tense during semi flexion and adduction of hip joint and relax during abducted hip joint
1.Capsule
2. Acetabular labrum
3. Transverse acetabular ligament
4. Ligamentum teres femoris (ligament of head of femur)
5. Ilio-femoral ligament
6. Pubo-femoral ligament
7. Ischio-femoral ligament
1. Capsule :
Capsule shows attachment medially near margins of acetabulum 5 to 6 mm above labrum and transverse acetabular ligament. Laterally shows attachment anteriorly on intertrochanteric line, posteriorly 1cm medial to intertrochanteric crest, above and below shows attachment on neck of femur close to greater trochanter and in front of lesser trochanter respectively. From intertrochanteric line few fibres of capsule goes medially along the neck forming retinacular fibres. Capsule is thick and strong anterosuperiorly but inferomedially weak. Deep fibres of capsule are circularly arranged while outer fibres are longitudinally arranged. Zona orbicularis are circularly arranged inner fibres of capsule around neck of femur.
Synovial membrane covers inner aspect of capsule, intracapsular part of femoral neck, acetabular labrum, transverse acetabular ligament, ligamentum teres and fat present in acetabular fossa. Synovial membrane may come out through a small gap on anterior aspect of capsule present in between pubo-femoral and ilio-femoral ligament.
2. Acetabular labrum
It is a cartilaginous rim showing attachment on margin of acetabulum. It is triangular in shape on cross section. Its functions are deepens the acetabular socket and hold head of femur tightly.
3. Transverse acetabular ligament
It is present in relation with acetabular notch bridging the notch. It is a noncartilagenous part of acetabular labrum. It converts acetabular notch into foramen for transmission of acetabular vessels and nerves to hip joint.
4. Ligamentum teres femoris (ligament of head of femur)
It is a triangular, flat and fibrous band. Its apex shows attachment on fovea present on femoral head. Base shows attachment on two margins of acetabular notch and it blends with transverse acetabular ligament. It is covered by synovial membrane. It become tense during semi flexion and adduction of hip joint and relax during abducted hip joint
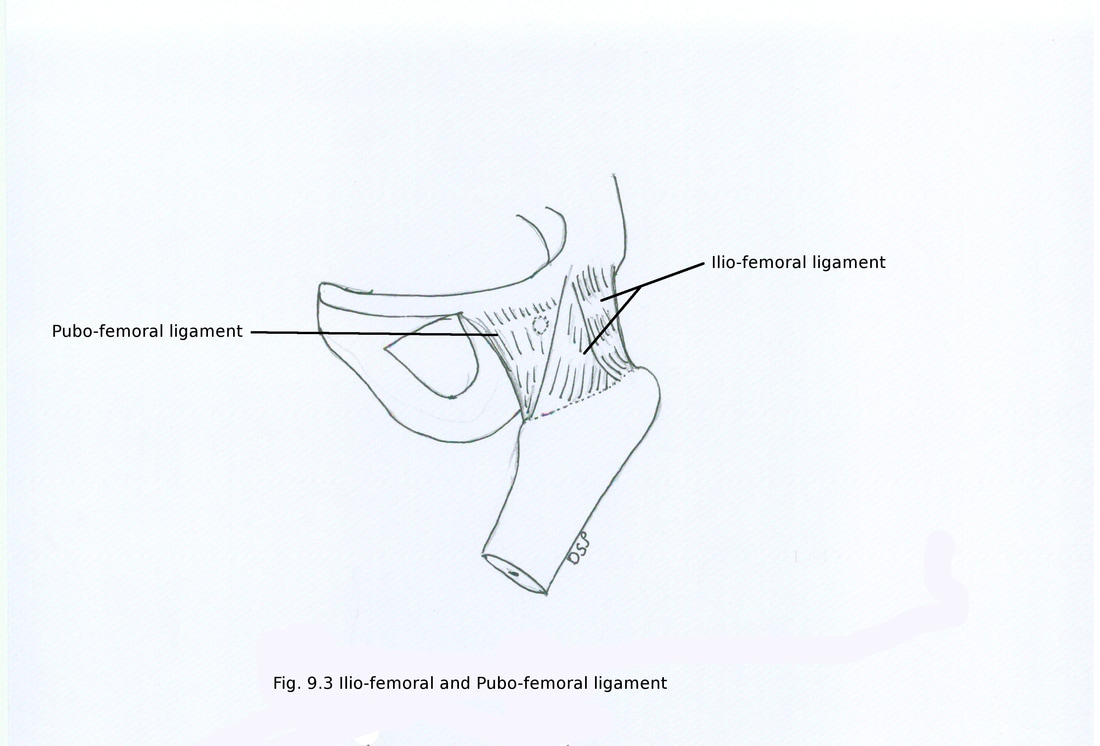
5. Ilio-femoral ligament
It is a strong ligament showing attachment on anterior aspect of capsule of hip joint. It is inverted Y shaped. Apex shows attachment on anterior inferior iliac spine while base shows attachment on intertrochanteric line. It shows three parts medial vertical band, lateral oblique band and intermediate thin part. Medial band shows attachment on lower part of intertrochanteric line, lateral band shows attachment on lateral part of intertrochanteric line and a small tubercle present in relation with that line and intermediate part shows attachment on rest of intertrochanteric line. Part of capsule of hip joint is made strong by it and it prevent hyperextension at hip joint.
6. Pubo-femoral ligament
It is a triangular ligament present on inferomedial aspect of joint capsule. Its base shows attachment on iliopubic eminence, superior pubic ramus, obturator membrane and obturator crest below it blends with capsule of joint and medial band of iliofemoral ligament.
It is a strong ligament showing attachment on anterior aspect of capsule of hip joint. It is inverted Y shaped. Apex shows attachment on anterior inferior iliac spine while base shows attachment on intertrochanteric line. It shows three parts medial vertical band, lateral oblique band and intermediate thin part. Medial band shows attachment on lower part of intertrochanteric line, lateral band shows attachment on lateral part of intertrochanteric line and a small tubercle present in relation with that line and intermediate part shows attachment on rest of intertrochanteric line. Part of capsule of hip joint is made strong by it and it prevent hyperextension at hip joint.
6. Pubo-femoral ligament
It is a triangular ligament present on inferomedial aspect of joint capsule. Its base shows attachment on iliopubic eminence, superior pubic ramus, obturator membrane and obturator crest below it blends with capsule of joint and medial band of iliofemoral ligament.
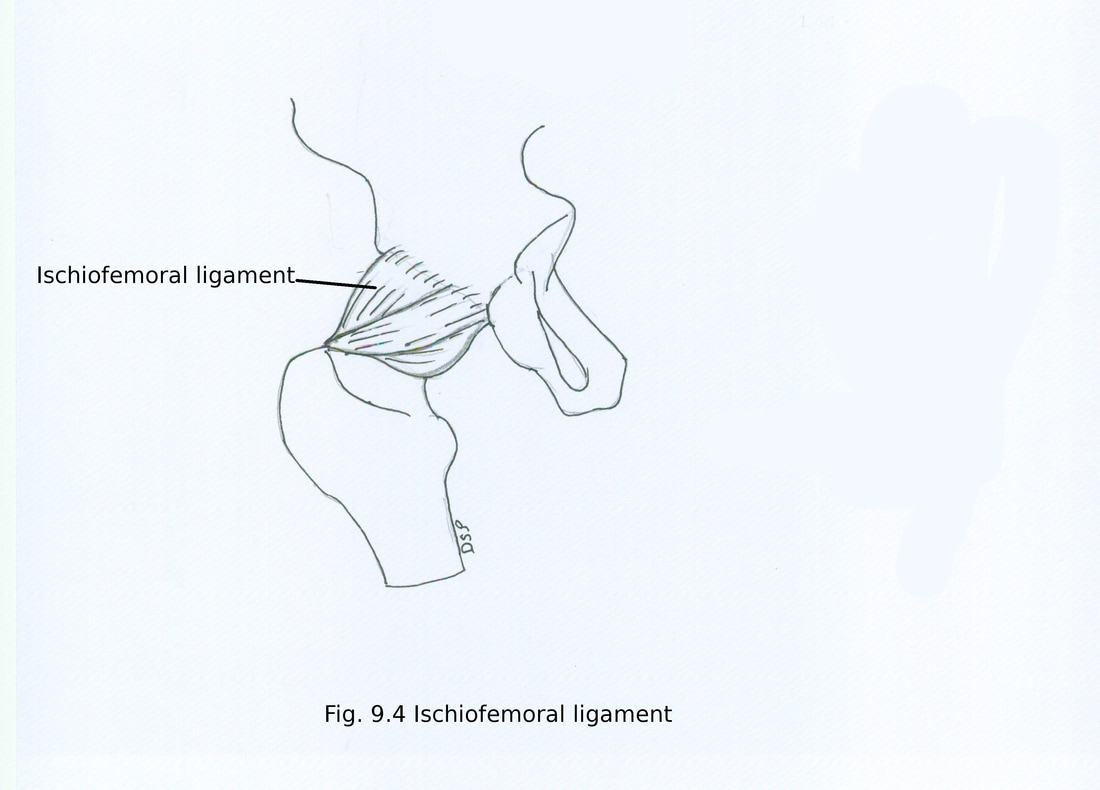
7. Ischio-femoral ligament
It is present on posterior aspect of capsule of hip joint to support capsule. It shows three parts central part or superior ischiofemoral part, lateral ischiofemoral part and medial ischiofemoral part. Central or superior part pass spirally upward and laterally behind neck of femur where it shows attachment on posteroinferior part on acetabular margin and below shows attachment on greater trochanter deep to iliofemoral ligament. Lateral and medial part covers posterior aspect of neck of femur which continue with zona orbicularis
It is present on posterior aspect of capsule of hip joint to support capsule. It shows three parts central part or superior ischiofemoral part, lateral ischiofemoral part and medial ischiofemoral part. Central or superior part pass spirally upward and laterally behind neck of femur where it shows attachment on posteroinferior part on acetabular margin and below shows attachment on greater trochanter deep to iliofemoral ligament. Lateral and medial part covers posterior aspect of neck of femur which continue with zona orbicularis
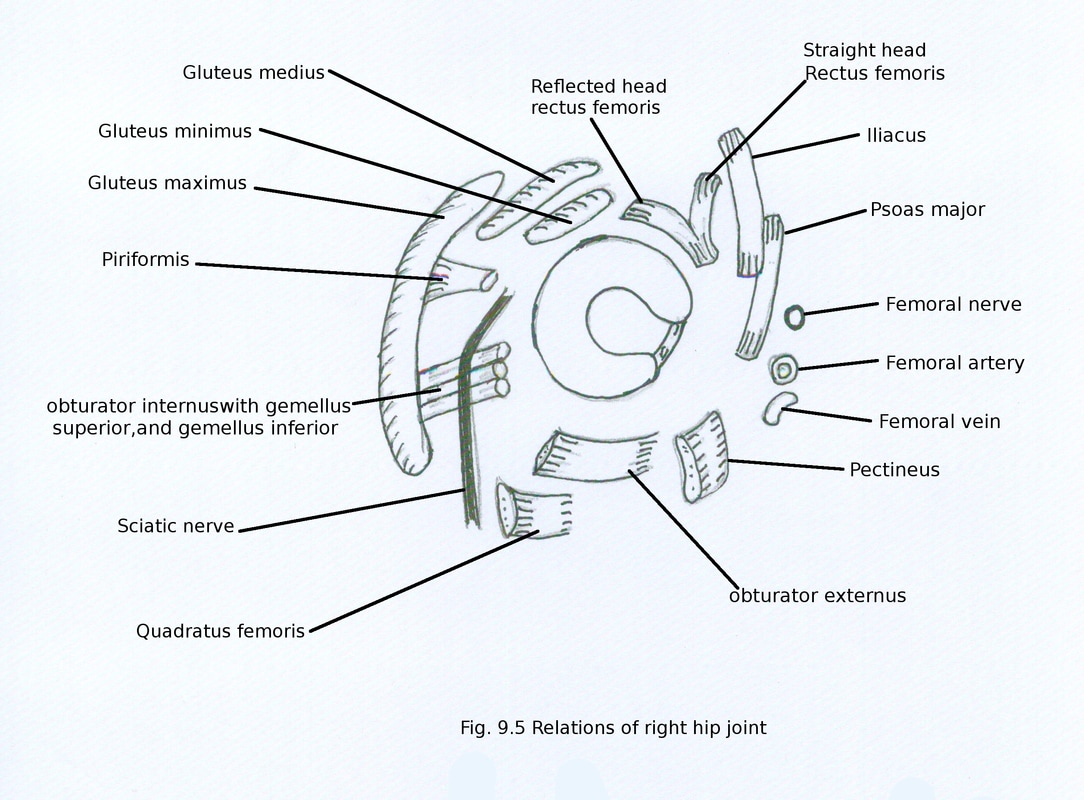
Relations :
Anteriorly: Iliacus, psoas major, straight head of rectus femoris and lateral part of pectineus muscle, femoral nerve in the groove between iliacus and psoas major, femoral artery anterior to tendon of psoas major and femoral vein anterior to pectineus muscle.
Posteriorly : Piriformis, obturator externus, obturator internus, gemellus superior, gemellus inferior, quadratus femoris and gluteus maximus muscles. Superior gluteal vessel and nerve inferior gluteal vessel and nerve above and below piriformis respectively, posterior femoral cutaneous nerve and nerve to quadratus femoris.
Superiorly : Medially reflected head of rectus femoris and laterally gluteus minimus muscles.
Inferiorly : Pectineus and obturator externus muscles
Anteriorly: Iliacus, psoas major, straight head of rectus femoris and lateral part of pectineus muscle, femoral nerve in the groove between iliacus and psoas major, femoral artery anterior to tendon of psoas major and femoral vein anterior to pectineus muscle.
Posteriorly : Piriformis, obturator externus, obturator internus, gemellus superior, gemellus inferior, quadratus femoris and gluteus maximus muscles. Superior gluteal vessel and nerve inferior gluteal vessel and nerve above and below piriformis respectively, posterior femoral cutaneous nerve and nerve to quadratus femoris.
Superiorly : Medially reflected head of rectus femoris and laterally gluteus minimus muscles.
Inferiorly : Pectineus and obturator externus muscles
Blood Supply :
Hip joint receive blood supply from branches of medial circumflex femoral artery, lateral circumflex femoral artery, obturator artery, superior gluteal artery and inferior gluteal artery. Branches from these arteries form cruciate anastomoses and trochanteric anastomoses.
Intracapsular part of neck and head of femur receive blood supply from 1) acetabular branches from obturator artery and medial circumflex femoral artery supplying acetabular fat and give medial epiphyseal artery which runs along with ligamentum teres to supply part of humeral head 2) Retinacular branches from medial circumflex femoral artery runs along with femoral neck through retinaculum of capsule and supply superior aspect of neck. It also gives out lateral epiphyseal artery supplying lateral part part of head. 3) few branches from medial circumflex femoral artery runs along with retinacular fibres of inferomedial aspect of neck to supply lower part of neck and head.
Nerve supply:
Hip joint is supplied by muscular branches of femoral nerve, obturator nerve, accessory obturator nerve, nerve to rectus femoris, nerve to quadratus femoris, superior gluteal nerve.
L2, L3,L4,L5 spinal segments control movements at hip joint. L2, L3 segments regulate flexion, adduction and medial rotation while L4, L5 regulate extension, abduction and lateral rotation.
Movements :
Movements which takes place at hip joint flexion, extension, adduction, abduction circumduction, medial and lateral rotation.
Flexion takes place around transverse axis. Flexion at hip joint which extended knee limited up to 90-100 degrees but may increase up to 120 degrees buy flexing knee joint. It is limited by contact of thigh with abdomen. Range of extension along the vertical line is 10-20 degrees and it is limited by tension of iliofemoral ligament.
Adduction and abduction take place along an anteroposterior axis which passes through the centre of head of femur. Adduction is limited by contact with opposite thigh. Adduction can be increased by semiflexion of hip joint. Abduction can take place up to 50 degree.
Medial and lateral rotation take place around a vertical axis. It passes through the centre of head of femur.
Circumduction is combination of all movements.
Muscles for movements:
Flexion: Iliacus, psoas major are chief flexors. Sartorius, pectineus and rectus femoris also help in flexion. Adductor longus help in flexion during initial face of flexion after full extension.
Extension: Gluteus maximus and hamstring muscles help in extension. Gluteus maximus acts during climbing and arising from bending position while hamstring muscles maintains extension in standing and walking.
Abduction: It is mainly by gluteus medius and minimus assisted by tensor fascia latae and sartorius. These muscles help in walking or running consistently.
Adduction : It is mainly by adductor longus, brevis and non-ischial part of adductor magnus. Assisted by medial part of pectineus and gracilis. Adduction is limited by contact with opposite thigh and can be increased by slightly flexing hip joint.
Lateral rotation : It is mainly by piriformis, obturator internus, obturator externus, superior and inferior gemelli, quadratus femoris and gluteus maximus.
Medial rotation : It is mainly by anterior fibres of gluteus medius and minimus and tensor fascia latae.
Applied anatomy :
1. Fracture of neck of femur : Occurs commonly in older persons. It is intracapsular in nature. Position of of limb laterally rotated and shortened. Types a) Sub capital (near head of femur) b) Cervical (middle part of neck) c) Basal (near trochanters) d) Pretrochanteric (distal to trochanters)
2. Lines to find out relative position of bony parts around hip joint are
a) Nelton's line : It is formed by joining anterior superior iliac spine and ischial tuberosity. This line passes through uppermost part of greater trochanter if greater trochanter lies above or below that line then fracture or dislocation of hip may be possible diagnosis.
b) Shenton’s line : It is a continuous curved line in x-ray of hip joint joining upper margin of obturator foramen and lower margin of neck of femur.
c) Schoemaker’s line: It is a straight line which passes through tip of greater trochanter, anterior superior iliac spine continue upward on anterior abdominal wall passing through umbilicus. If greater trochanter is elevated then line will pass below umbilicus.
d) Bryant's line : It is a line between uppermost point of greater trochanter and a horizontal line which passes through anterior superior iliac spine. It is normally 5 centimeter. Increase or decrease in it indicate dislocation of hip joint or any other deformity.
3. Congenital dislocation : Hip joint dislocates commonly to gluteal surface of ilium. It is
common in girls.
Hip joint receive blood supply from branches of medial circumflex femoral artery, lateral circumflex femoral artery, obturator artery, superior gluteal artery and inferior gluteal artery. Branches from these arteries form cruciate anastomoses and trochanteric anastomoses.
Intracapsular part of neck and head of femur receive blood supply from 1) acetabular branches from obturator artery and medial circumflex femoral artery supplying acetabular fat and give medial epiphyseal artery which runs along with ligamentum teres to supply part of humeral head 2) Retinacular branches from medial circumflex femoral artery runs along with femoral neck through retinaculum of capsule and supply superior aspect of neck. It also gives out lateral epiphyseal artery supplying lateral part part of head. 3) few branches from medial circumflex femoral artery runs along with retinacular fibres of inferomedial aspect of neck to supply lower part of neck and head.
Nerve supply:
Hip joint is supplied by muscular branches of femoral nerve, obturator nerve, accessory obturator nerve, nerve to rectus femoris, nerve to quadratus femoris, superior gluteal nerve.
L2, L3,L4,L5 spinal segments control movements at hip joint. L2, L3 segments regulate flexion, adduction and medial rotation while L4, L5 regulate extension, abduction and lateral rotation.
Movements :
Movements which takes place at hip joint flexion, extension, adduction, abduction circumduction, medial and lateral rotation.
Flexion takes place around transverse axis. Flexion at hip joint which extended knee limited up to 90-100 degrees but may increase up to 120 degrees buy flexing knee joint. It is limited by contact of thigh with abdomen. Range of extension along the vertical line is 10-20 degrees and it is limited by tension of iliofemoral ligament.
Adduction and abduction take place along an anteroposterior axis which passes through the centre of head of femur. Adduction is limited by contact with opposite thigh. Adduction can be increased by semiflexion of hip joint. Abduction can take place up to 50 degree.
Medial and lateral rotation take place around a vertical axis. It passes through the centre of head of femur.
Circumduction is combination of all movements.
Muscles for movements:
Flexion: Iliacus, psoas major are chief flexors. Sartorius, pectineus and rectus femoris also help in flexion. Adductor longus help in flexion during initial face of flexion after full extension.
Extension: Gluteus maximus and hamstring muscles help in extension. Gluteus maximus acts during climbing and arising from bending position while hamstring muscles maintains extension in standing and walking.
Abduction: It is mainly by gluteus medius and minimus assisted by tensor fascia latae and sartorius. These muscles help in walking or running consistently.
Adduction : It is mainly by adductor longus, brevis and non-ischial part of adductor magnus. Assisted by medial part of pectineus and gracilis. Adduction is limited by contact with opposite thigh and can be increased by slightly flexing hip joint.
Lateral rotation : It is mainly by piriformis, obturator internus, obturator externus, superior and inferior gemelli, quadratus femoris and gluteus maximus.
Medial rotation : It is mainly by anterior fibres of gluteus medius and minimus and tensor fascia latae.
Applied anatomy :
1. Fracture of neck of femur : Occurs commonly in older persons. It is intracapsular in nature. Position of of limb laterally rotated and shortened. Types a) Sub capital (near head of femur) b) Cervical (middle part of neck) c) Basal (near trochanters) d) Pretrochanteric (distal to trochanters)
2. Lines to find out relative position of bony parts around hip joint are
a) Nelton's line : It is formed by joining anterior superior iliac spine and ischial tuberosity. This line passes through uppermost part of greater trochanter if greater trochanter lies above or below that line then fracture or dislocation of hip may be possible diagnosis.
b) Shenton’s line : It is a continuous curved line in x-ray of hip joint joining upper margin of obturator foramen and lower margin of neck of femur.
c) Schoemaker’s line: It is a straight line which passes through tip of greater trochanter, anterior superior iliac spine continue upward on anterior abdominal wall passing through umbilicus. If greater trochanter is elevated then line will pass below umbilicus.
d) Bryant's line : It is a line between uppermost point of greater trochanter and a horizontal line which passes through anterior superior iliac spine. It is normally 5 centimeter. Increase or decrease in it indicate dislocation of hip joint or any other deformity.
3. Congenital dislocation : Hip joint dislocates commonly to gluteal surface of ilium. It is
common in girls.
Ligaments :
1. Capsule :
Upper attachment on femur : Capsule shows attachment on lower end of femur posteriorly on upper margins of intercondylar notch and margins of medial and lateral femoral condyles. Medially shows attachment on a line just 1cm above articular margin of medial condyle. Laterally shows attachment on a line just 1cm above articular margin of lateral condyle enclosing origin of popliteus. Anteriorly it is deficient communicating with suprapatellar bursa.
Lower attachment on tibia : Below it shows attachment 1 cm away from articular margin of tibial condyles. Posteriorly in relation with lateral condyle it is deficient for passage of tendon of popliteus. Anteriorly it extends down shows attachment on margin of triangular area in relation with tibial tuberosity finally blends with ligamentum patellae.
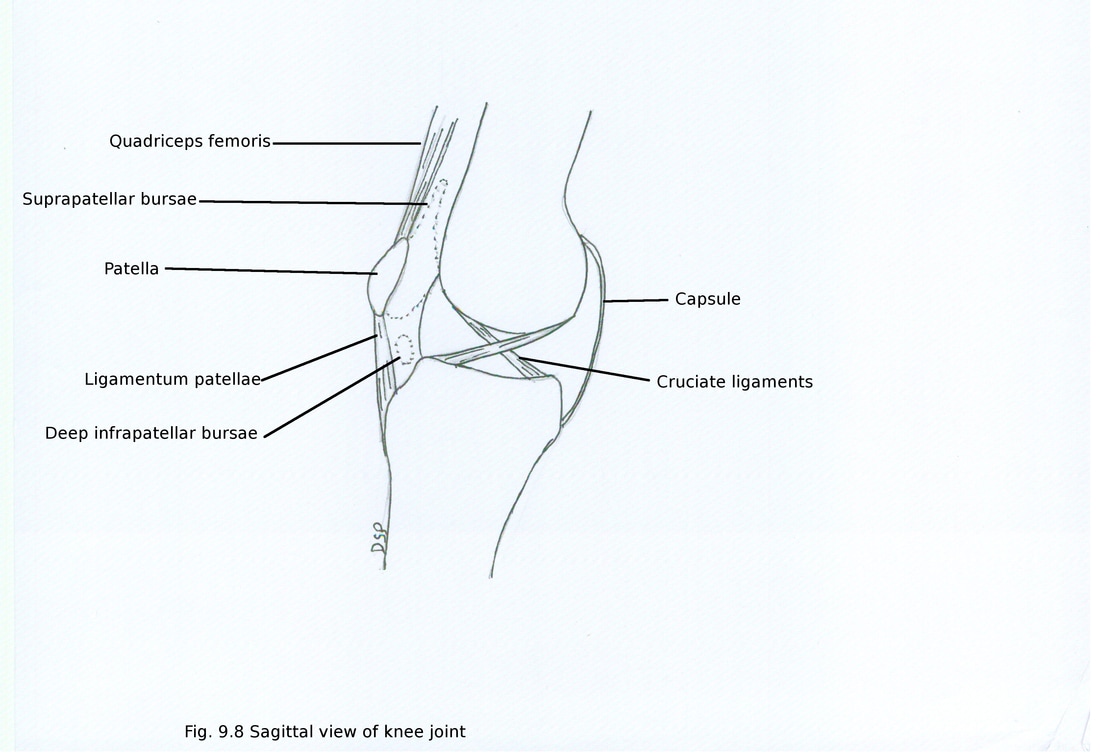
2. Ligamentum patellae
It is part of tendon of quadriceps femoris muscle. It is 6-8cm in length. It extended from apex of patella to upper part of tibial tuberosity. It shows attachment on rough anterior surface, margin, depression on posterior surface and apex of patella above. Below shows attachment on smooth upper part of tibial tuberosity. Subcutaneous and deep infrapatellar bursae lies in relation with it.
3. Tibial and fibular collateral ligaments
Tibial collateral ligament has superficial and deep parts. Having attachment on medial epicondyle of femur. Deep part below shows attachment on upper margin of medial condyle of tibia in relation with groove for semimembranosus muscle. Deep part also shows attachment on outer margin of medial meniscus. Finally it blends with capsule of knee joint. Superficial part goes downwards forwards shows attachment on upper part of medial border of shaft of tibia. Inferior medial genicular vessels and nerve lies deep to it.
Fibular collateral ligament shows attachment on lateral epicondyle of femur and head of fibula. It goes downwards and backwards. Tendon of biceps femoris lies superficial to it.
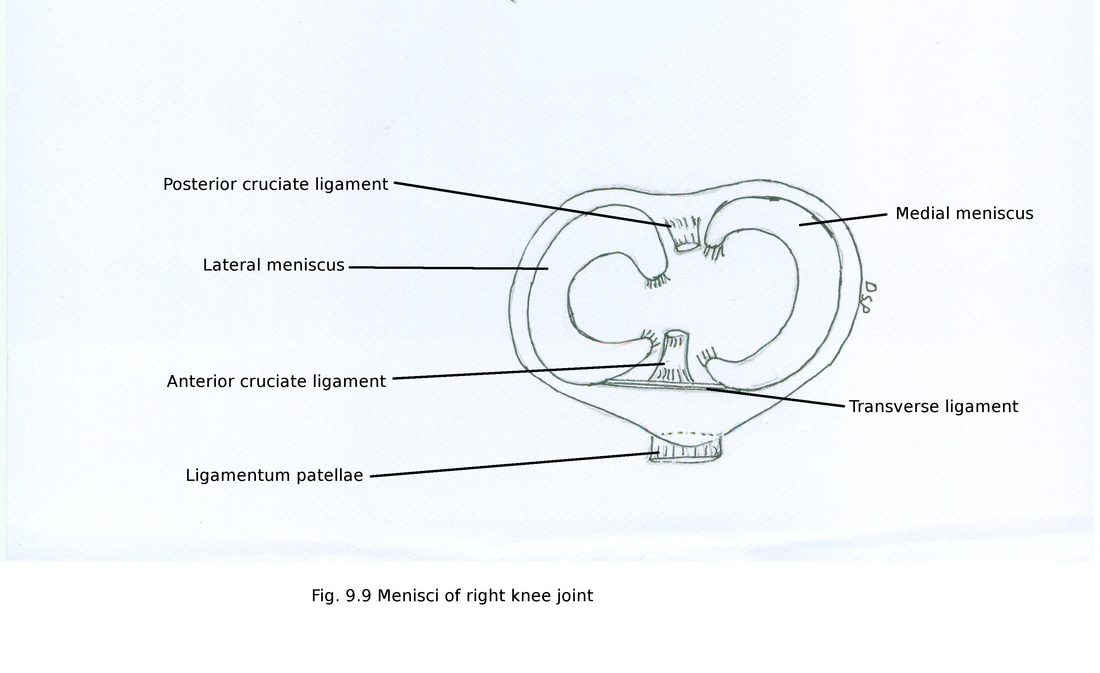
4. Anterior and posterior cruciate ligaments
These two ligaments are intracapsular. They cross each other in “X” like manner.
Anterior cruciate ligament below show attachment on anterior part of intercondylar area of tibia and above on posterior part of medial surface of lateral condyle of femur. It goes upward backward and laterally. It is about 3.8 cm in length and 1.1 cm width. It becomes taut during extension of knee. It prevents posterior dislocation of femur on tibia.
Posterior cruciate ligament more thick and strong. Below it show attachment on posterior part of intercondylar area of tibia and above on anterior part of lateral surface of medial condyle of femur. It goes upward forward and medially. It is about 3.8 cm in length and 1.3 cm width. It becomes taut during flexion of knee. It prevents anterior dislocation of femur on tibia.
1. Capsule :
Upper attachment on femur : Capsule shows attachment on lower end of femur posteriorly on upper margins of intercondylar notch and margins of medial and lateral femoral condyles. Medially shows attachment on a line just 1cm above articular margin of medial condyle. Laterally shows attachment on a line just 1cm above articular margin of lateral condyle enclosing origin of popliteus. Anteriorly it is deficient communicating with suprapatellar bursa.
Lower attachment on tibia : Below it shows attachment 1 cm away from articular margin of tibial condyles. Posteriorly in relation with lateral condyle it is deficient for passage of tendon of popliteus. Anteriorly it extends down shows attachment on margin of triangular area in relation with tibial tuberosity finally blends with ligamentum patellae.
2. Ligamentum patellae
It is part of tendon of quadriceps femoris muscle. It is 6-8cm in length. It extended from apex of patella to upper part of tibial tuberosity. It shows attachment on rough anterior surface, margin, depression on posterior surface and apex of patella above. Below shows attachment on smooth upper part of tibial tuberosity. Subcutaneous and deep infrapatellar bursae lies in relation with it.
3. Tibial and fibular collateral ligaments
Tibial collateral ligament has superficial and deep parts. Having attachment on medial epicondyle of femur. Deep part below shows attachment on upper margin of medial condyle of tibia in relation with groove for semimembranosus muscle. Deep part also shows attachment on outer margin of medial meniscus. Finally it blends with capsule of knee joint. Superficial part goes downwards forwards shows attachment on upper part of medial border of shaft of tibia. Inferior medial genicular vessels and nerve lies deep to it.
Fibular collateral ligament shows attachment on lateral epicondyle of femur and head of fibula. It goes downwards and backwards. Tendon of biceps femoris lies superficial to it.
4. Anterior and posterior cruciate ligaments
These two ligaments are intracapsular. They cross each other in “X” like manner.
Anterior cruciate ligament below show attachment on anterior part of intercondylar area of tibia and above on posterior part of medial surface of lateral condyle of femur. It goes upward backward and laterally. It is about 3.8 cm in length and 1.1 cm width. It becomes taut during extension of knee. It prevents posterior dislocation of femur on tibia.
Posterior cruciate ligament more thick and strong. Below it show attachment on posterior part of intercondylar area of tibia and above on anterior part of lateral surface of medial condyle of femur. It goes upward forward and medially. It is about 3.8 cm in length and 1.3 cm width. It becomes taut during flexion of knee. It prevents anterior dislocation of femur on tibia.
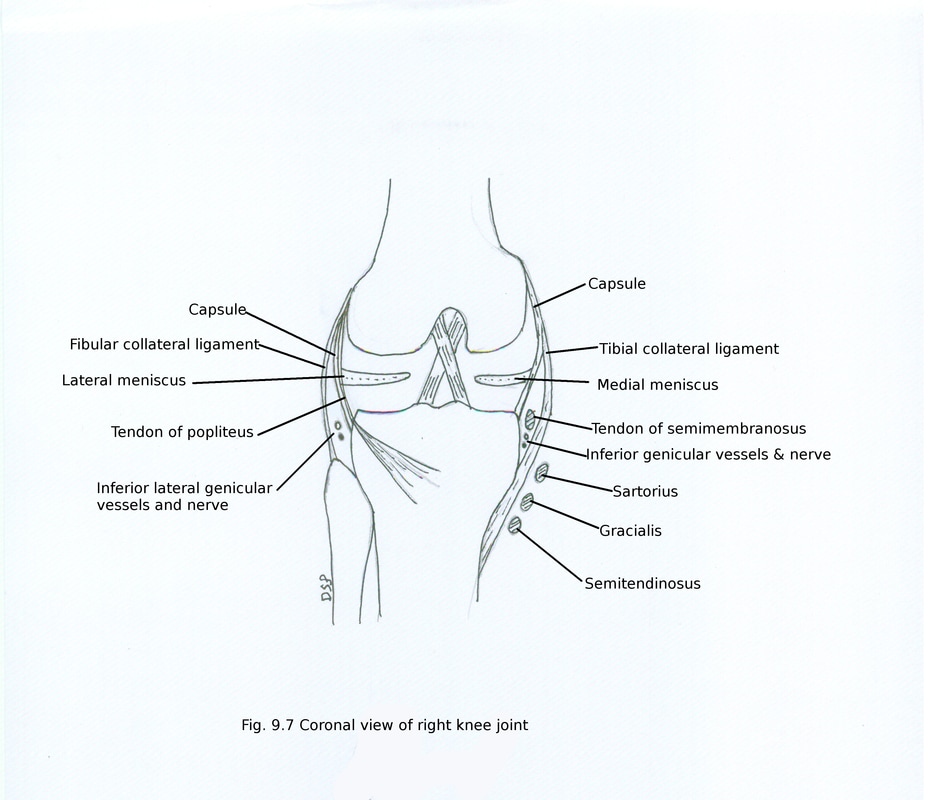
5. Medial and lateral meniscus
These are intra-articular fibro-cartilagenous discs between condyles of femur and tibia. It divides joint cavity into upper and lower compartment.
Medial meniscus having semilunar shape. Antero-posterior length is more as compared to lateral meniscus. It is broad posteriorly. It shows two surfaces upper and lower, two margins medial and lateral, two horns anterior and posterior. Upper surface concave in shape while lower surface is flat. Medial margin convex medially and thick shows attachment on capsule and tibial collateral ligament. Attachment on tibia known as coronary ligament. Lateral margin concave laterally and thin. Horns shows attachment on intercondylar area of tibia. Medial meniscus is more prone to injury.
Lateral meniscus circular in shape forming four fifth of a circle. It covers more area. Posteriorly tendon of popliteus forms a groove on it. It shows two surfaces upper and lower, two margins medial and lateral, two horns anterior and posterior. Upper surface concave in shape while lower surface is flat. Medial margin concave medially and thin. Lateral margin thick and convex laterally show attachment on capsule. Posterior horn shows attachment of menisco-femoral ligaments and fibres of popliteus. Horns shows attachment on intercondylar area of tibia.
Functions of menisci : Menisci increases concavity of condyles of tibia. It absorb shock. Help in flushing of synovial fluid inside knee joint.
These are intra-articular fibro-cartilagenous discs between condyles of femur and tibia. It divides joint cavity into upper and lower compartment.
Medial meniscus having semilunar shape. Antero-posterior length is more as compared to lateral meniscus. It is broad posteriorly. It shows two surfaces upper and lower, two margins medial and lateral, two horns anterior and posterior. Upper surface concave in shape while lower surface is flat. Medial margin convex medially and thick shows attachment on capsule and tibial collateral ligament. Attachment on tibia known as coronary ligament. Lateral margin concave laterally and thin. Horns shows attachment on intercondylar area of tibia. Medial meniscus is more prone to injury.
Lateral meniscus circular in shape forming four fifth of a circle. It covers more area. Posteriorly tendon of popliteus forms a groove on it. It shows two surfaces upper and lower, two margins medial and lateral, two horns anterior and posterior. Upper surface concave in shape while lower surface is flat. Medial margin concave medially and thin. Lateral margin thick and convex laterally show attachment on capsule. Posterior horn shows attachment of menisco-femoral ligaments and fibres of popliteus. Horns shows attachment on intercondylar area of tibia.
Functions of menisci : Menisci increases concavity of condyles of tibia. It absorb shock. Help in flushing of synovial fluid inside knee joint.
6. Oblique popliteal ligament
Semimembranosus tendon gives an extension from its insertion as oblique popliteal ligament. It goes upward laterally from posterior surface of medial condyle of tibia to lateral part of intercondylar line of femur. It finally fuse with capsule of knee forming floor of popliteal fossa. Middle genicular vessels and nerve, genicular branch of posterior division of obturator nerve pierce it.
7. Arcuate popliteal ligament
It is fibrous and Y shaped. Stem of Y shows attachment on styloid process of head of fibula. Posterior band arches over tendon of popliteus and shows attachment on lateral condyle of tibia. Anterior band goes deep to fibular collateral ligament and shows attachment on lateral condyle of femur.
8. Coronary ligament
It is part of capsule of knee joint where medial and lateral meniscus attached to capsule on its outer margin.
9. Transverse ligament
It is transversely located connecting anterior ends of medial and lateral meniscus.
10. Menisco femoral ligament
Medial condyle of femur shows connection with posterior horn of lateral meniscus by anterior and posterior menisco-femoral ligaments. Anterior ligament lies anterior to posterior cruciate ligament and posterior ligament lies posterior to posterior cruciate ligament.
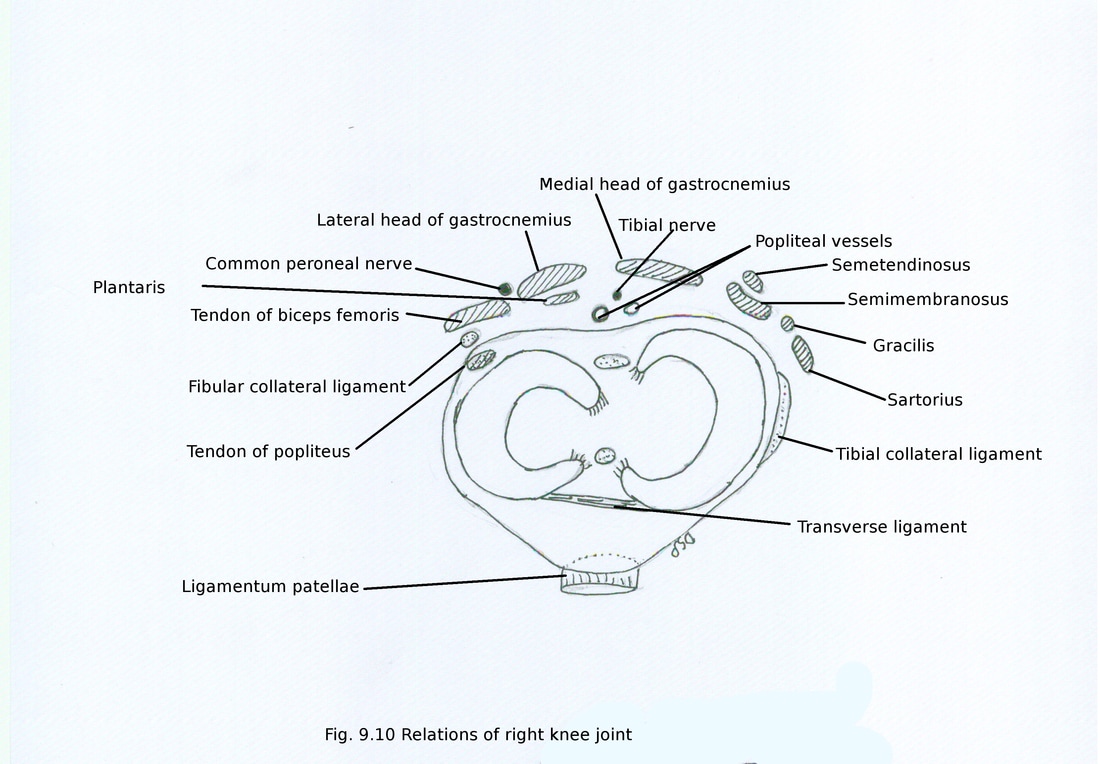
Relations of knee joint :
Anteriorly : Quadriceps femoris, patella, ligamentum patellae, prepatellar bursae and patellar plexus
Antero-medially : Medial patellar retinaculum
Antero-laterally : Lateral patellar retinaculum and iliotibial tract
Posteriorly : Popliteal vessels, tibial nerve, plantaris, medial and lateral heads of gastrocnemius and oblique popliteal ligament
Postero-medially : Sartorius, gracilis, semimembranosus, semetendinosus
Postero-laterally : Tendon of biceps femoris and common peroneal nerve.
Semimembranosus tendon gives an extension from its insertion as oblique popliteal ligament. It goes upward laterally from posterior surface of medial condyle of tibia to lateral part of intercondylar line of femur. It finally fuse with capsule of knee forming floor of popliteal fossa. Middle genicular vessels and nerve, genicular branch of posterior division of obturator nerve pierce it.
7. Arcuate popliteal ligament
It is fibrous and Y shaped. Stem of Y shows attachment on styloid process of head of fibula. Posterior band arches over tendon of popliteus and shows attachment on lateral condyle of tibia. Anterior band goes deep to fibular collateral ligament and shows attachment on lateral condyle of femur.
8. Coronary ligament
It is part of capsule of knee joint where medial and lateral meniscus attached to capsule on its outer margin.
9. Transverse ligament
It is transversely located connecting anterior ends of medial and lateral meniscus.
10. Menisco femoral ligament
Medial condyle of femur shows connection with posterior horn of lateral meniscus by anterior and posterior menisco-femoral ligaments. Anterior ligament lies anterior to posterior cruciate ligament and posterior ligament lies posterior to posterior cruciate ligament.
Relations of knee joint :
Anteriorly : Quadriceps femoris, patella, ligamentum patellae, prepatellar bursae and patellar plexus
Antero-medially : Medial patellar retinaculum
Antero-laterally : Lateral patellar retinaculum and iliotibial tract
Posteriorly : Popliteal vessels, tibial nerve, plantaris, medial and lateral heads of gastrocnemius and oblique popliteal ligament
Postero-medially : Sartorius, gracilis, semimembranosus, semetendinosus
Postero-laterally : Tendon of biceps femoris and common peroneal nerve.
Bursae around knee joint :
There are about 12 bursae around knee joint.
Anterior bursae : These are four in number.
Subcutaneous prepatellar bursae : It lies anterior to lower part of patella deep to skin. Housemaid’s knee is a condition in which inflammation and swelling of prepatellar bursae takes place. In housemaid this is common because of kneel-down position of housemaid during scrubbing of floor. This position causes friction of bursae against patella.
Subcutaneous infrapatellar bursae : It lies in between skin and lower part of tibial tuberosity. Clergyman’s bursa is a condition in which inflammation and swelling of subcutaneous infrapatellar bursae takes place. In clergyman this is common because of kneel-down position during praying with trunk upright. This position causes friction of bursae against tibial tuberosity.
Deep infrapatellar bursae : It lies deep to ligamentum patellae between ligamentum patellae and tibial tuberosity.
Supra patellar bursae : It lies deep to quadriceps femoris between quadriceps femoris and lower part of femur.
Lateral bursae :
1) Between lateral head of gastrocnemius and capsule of knee joint.
2) Between tendon of biceps femoris and fibular collateral ligament.
3) Between fibular collateral ligament and tendon of popliteus.
4) Between lateral condyle of femur and tendon of popliteus.
Medial bursae :
1) Between medial head of gastrocnemius and capsule of knee joint.
2) Between superficial part of tibial collateral ligament and three muscles sartorius, gracilis and semitendinosus.
3) Between superficial and deep part of tibial collateral ligament.
4) Between insertion of semimembranosus and medial condyle of tibia.
Posterior bursae : These are present or may be absent.
Blood Supply:
It receives blood supply from anastomosis around knee joint formed by a) five genicular branches from popliteal artery (superior, middle and inferior genicular branches) b) descending genicular branch of femoral artery c) descending branch of lateral circumflex femoral artery d) recurrent branches of anterior tibial artery and e) circumflex fibular branch of posterior tibial artery.
Nerve supply:
It receives nerve from three branches of femoral nerve (through branches to three vastus muscle), three branches of tibial nerve (superior medial genicular, inferior medial genicular and middle genicular nerve), three from common peroneal nerve ( superior lateral genicular, inferior lateral genicular and recurrent genicular), genicular branch of obturator nerve.
Muscles for movements :
Movements which takes place at knee joint are flexion, extension, medial rotation and lateral rotation.
Extension causes straightening of leg at knee joint. After full extension joint becomes close packed known as locked. Knee can extend 5-10 degree beyond vertical axis.
Flexion of knee can takes place up to 120 degree in an extended hip, with flexed knee can extend up to 140 degree and can be flexed passively up to 160 degree.
Medial and lateral rotation are conjunct or adjunct. Automatic rotation during flexion and extension is conjunct rotation up to 20 degree. Active contraction of muscles causes adjunct rotation takes place in semi flexed knee up to 50-70 degree.
Movements at knee joint from full flexed position to full extension (locking of knee joint) :
In fully flexed knee joint posterior parts of femoral condyles comes in contact with posterior horns of medial and lateral meniscus. When extension starts femoral condyles roll forwards over the surface of menisci. This rolling causes transverse axis at joint to move forward. This movement stopped by fibrous capsule (posterior part), posterior cruciate ligament and oblique popliteal ligament. Then both femoral condyles spin forward on upper surface of menisci. As lateral meniscus is shorter than medial meniscus lateral femoral condyle reaches anterior horn of lateral meniscus early. It fully cover lateral menisco-femoral compartment. But extension is not yet completed and anterior horn of medial meniscus not covered by medial femoral condyle. Anterior cruciate ligament acts as a vertical axis around which medial femoral condyle rotates medially and backward to reach anterior horn of medial meniscus. At the same time lateral femoral condyle with lateral meniscus glide forward in lateral menisco-tibial compartment. This movement covers last 30 degree of extension. This causes locking of knee joint and method is locking of knee joint. After locking of knee joint all ligaments are stretched, all surfaces are in maximum contact and with any active contraction of extensor muscle. All these movements takes place when foot is on the ground.
Exact opposite takes place while unlocking. Popliteus help in unlocking of knee joint.
Flexion : Chief muscle for flexion are semimembranosus, semitendinosus, biceps femoris assisted by popliteus (initiate), sartorius, gracilis, gastrocnemius, plantaris
Extension : Chief extensor are quadriceps femoris assisted by tensor fascia latae
Medial rotation : Chief muscles for medial rotation are semimembranosus, semitendinosus, popliteus assisted by sartorius, gracilis
Lateral rotation : Chief muscle for lateral rotation are biceps femoris and assisted by gluteus maximus and tensor fascia latae.
Applied anatomy :
1. Injury to medial meniscus is common because fibres of popliteus pull posterior horn of lateral meniscus backward and avoid injury to it by crushing, range of movement is more in lateral meniscus.
2. Arthritis of knee joint is common mainly affecting aged women. Causes painful movements and limit movements at knee joint.
3. Anterior cruciate ligament ruptured commonly causing excessive anterior movement of tibia. Rupture of both cruciate ligament causes increase in forward and backward movement of tibia.
4. Arthroscopy is a method to see interior of knee joint by endoscope.
5. Knee replacement is a method to replace damaged arthritic knee joint by artificial knee joint.
There are about 12 bursae around knee joint.
Anterior bursae : These are four in number.
Subcutaneous prepatellar bursae : It lies anterior to lower part of patella deep to skin. Housemaid’s knee is a condition in which inflammation and swelling of prepatellar bursae takes place. In housemaid this is common because of kneel-down position of housemaid during scrubbing of floor. This position causes friction of bursae against patella.
Subcutaneous infrapatellar bursae : It lies in between skin and lower part of tibial tuberosity. Clergyman’s bursa is a condition in which inflammation and swelling of subcutaneous infrapatellar bursae takes place. In clergyman this is common because of kneel-down position during praying with trunk upright. This position causes friction of bursae against tibial tuberosity.
Deep infrapatellar bursae : It lies deep to ligamentum patellae between ligamentum patellae and tibial tuberosity.
Supra patellar bursae : It lies deep to quadriceps femoris between quadriceps femoris and lower part of femur.
Lateral bursae :
1) Between lateral head of gastrocnemius and capsule of knee joint.
2) Between tendon of biceps femoris and fibular collateral ligament.
3) Between fibular collateral ligament and tendon of popliteus.
4) Between lateral condyle of femur and tendon of popliteus.
Medial bursae :
1) Between medial head of gastrocnemius and capsule of knee joint.
2) Between superficial part of tibial collateral ligament and three muscles sartorius, gracilis and semitendinosus.
3) Between superficial and deep part of tibial collateral ligament.
4) Between insertion of semimembranosus and medial condyle of tibia.
Posterior bursae : These are present or may be absent.
Blood Supply:
It receives blood supply from anastomosis around knee joint formed by a) five genicular branches from popliteal artery (superior, middle and inferior genicular branches) b) descending genicular branch of femoral artery c) descending branch of lateral circumflex femoral artery d) recurrent branches of anterior tibial artery and e) circumflex fibular branch of posterior tibial artery.
Nerve supply:
It receives nerve from three branches of femoral nerve (through branches to three vastus muscle), three branches of tibial nerve (superior medial genicular, inferior medial genicular and middle genicular nerve), three from common peroneal nerve ( superior lateral genicular, inferior lateral genicular and recurrent genicular), genicular branch of obturator nerve.
Muscles for movements :
Movements which takes place at knee joint are flexion, extension, medial rotation and lateral rotation.
Extension causes straightening of leg at knee joint. After full extension joint becomes close packed known as locked. Knee can extend 5-10 degree beyond vertical axis.
Flexion of knee can takes place up to 120 degree in an extended hip, with flexed knee can extend up to 140 degree and can be flexed passively up to 160 degree.
Medial and lateral rotation are conjunct or adjunct. Automatic rotation during flexion and extension is conjunct rotation up to 20 degree. Active contraction of muscles causes adjunct rotation takes place in semi flexed knee up to 50-70 degree.
Movements at knee joint from full flexed position to full extension (locking of knee joint) :
In fully flexed knee joint posterior parts of femoral condyles comes in contact with posterior horns of medial and lateral meniscus. When extension starts femoral condyles roll forwards over the surface of menisci. This rolling causes transverse axis at joint to move forward. This movement stopped by fibrous capsule (posterior part), posterior cruciate ligament and oblique popliteal ligament. Then both femoral condyles spin forward on upper surface of menisci. As lateral meniscus is shorter than medial meniscus lateral femoral condyle reaches anterior horn of lateral meniscus early. It fully cover lateral menisco-femoral compartment. But extension is not yet completed and anterior horn of medial meniscus not covered by medial femoral condyle. Anterior cruciate ligament acts as a vertical axis around which medial femoral condyle rotates medially and backward to reach anterior horn of medial meniscus. At the same time lateral femoral condyle with lateral meniscus glide forward in lateral menisco-tibial compartment. This movement covers last 30 degree of extension. This causes locking of knee joint and method is locking of knee joint. After locking of knee joint all ligaments are stretched, all surfaces are in maximum contact and with any active contraction of extensor muscle. All these movements takes place when foot is on the ground.
Exact opposite takes place while unlocking. Popliteus help in unlocking of knee joint.
Flexion : Chief muscle for flexion are semimembranosus, semitendinosus, biceps femoris assisted by popliteus (initiate), sartorius, gracilis, gastrocnemius, plantaris
Extension : Chief extensor are quadriceps femoris assisted by tensor fascia latae
Medial rotation : Chief muscles for medial rotation are semimembranosus, semitendinosus, popliteus assisted by sartorius, gracilis
Lateral rotation : Chief muscle for lateral rotation are biceps femoris and assisted by gluteus maximus and tensor fascia latae.
Applied anatomy :
1. Injury to medial meniscus is common because fibres of popliteus pull posterior horn of lateral meniscus backward and avoid injury to it by crushing, range of movement is more in lateral meniscus.
2. Arthritis of knee joint is common mainly affecting aged women. Causes painful movements and limit movements at knee joint.
3. Anterior cruciate ligament ruptured commonly causing excessive anterior movement of tibia. Rupture of both cruciate ligament causes increase in forward and backward movement of tibia.
4. Arthroscopy is a method to see interior of knee joint by endoscope.
5. Knee replacement is a method to replace damaged arthritic knee joint by artificial knee joint.
TIBIO-FIBULAR JOINTS
SUPERIOR TIBIO-FIBULAR JOINT
It is a plane synovial type of joint.
Bones forming joints are circular articular facet present on postero-lateral part of lateral condyle of tibia and head of fibula. These bones are covered by capsule.
Nerve supply is supplied by a branch from common peroneal nerve and nerve to popliteus.
Movements takes place at this joint are gliding in dorsi-flexion of foot.
MIDDLE TIBIO-FIBULAR JOINT
It is a fibrous type of joint.
Formed by interosseous membrane connecting interosseous borders of tibia and fibula. Interosseous membrane shows fibres having direction downward and laterally. It forms a upper free margin above which anterior tibial vessels goes to anterior compartment of leg. In lower part this membrane is pierced by perforating branch of peroneal artery.
INFERIOR TIBIO-FIBULAR JOINT
It is a syndesmosis type of fibrous joint.
Bones forming joints are triangular articular concave surface present on lower part of tibia and triangular articular rough part of lower end of fibula. Anterior and posterior tibio-fibular ligament and interosseous ligament are present in relation with it. Interosseous ligament is a strong band like connecting rough surface of tibia and fibula continuous above with interosseous membrane. Anterior tibio-fibular ligament goes downward and laterally in front of interosseous ligament. Posterior tibio-fibular ligament goes downward and laterally behind interosseous ligament.
Synovial membrane of ankle joint extends into lower part of inferior tibio-fibular joint.
Nerve supply is supplied by a branches from deep peroneal nerve and sural nerve.
SUPERIOR TIBIO-FIBULAR JOINT
It is a plane synovial type of joint.
Bones forming joints are circular articular facet present on postero-lateral part of lateral condyle of tibia and head of fibula. These bones are covered by capsule.
Nerve supply is supplied by a branch from common peroneal nerve and nerve to popliteus.
Movements takes place at this joint are gliding in dorsi-flexion of foot.
MIDDLE TIBIO-FIBULAR JOINT
It is a fibrous type of joint.
Formed by interosseous membrane connecting interosseous borders of tibia and fibula. Interosseous membrane shows fibres having direction downward and laterally. It forms a upper free margin above which anterior tibial vessels goes to anterior compartment of leg. In lower part this membrane is pierced by perforating branch of peroneal artery.
INFERIOR TIBIO-FIBULAR JOINT
It is a syndesmosis type of fibrous joint.
Bones forming joints are triangular articular concave surface present on lower part of tibia and triangular articular rough part of lower end of fibula. Anterior and posterior tibio-fibular ligament and interosseous ligament are present in relation with it. Interosseous ligament is a strong band like connecting rough surface of tibia and fibula continuous above with interosseous membrane. Anterior tibio-fibular ligament goes downward and laterally in front of interosseous ligament. Posterior tibio-fibular ligament goes downward and laterally behind interosseous ligament.
Synovial membrane of ankle joint extends into lower part of inferior tibio-fibular joint.
Nerve supply is supplied by a branches from deep peroneal nerve and sural nerve.
ANKLE JOINT
It is a synovial type of joint hinge variety.
Bones forming joints :
Above lower articular surface of lower end of tibia, medial malleolus of tibia, lateral malleolus of fibula and inferior transverse tibio-fibular ligament. All these structures together forms a tibio-fibular socket or tibio-fibular mortise.
Below upper surface of body of talus, medially comma shaped facet for medial malleolus and laterally triangular facet of talus for lateral malleolus
It is a synovial type of joint hinge variety.
Bones forming joints :
Above lower articular surface of lower end of tibia, medial malleolus of tibia, lateral malleolus of fibula and inferior transverse tibio-fibular ligament. All these structures together forms a tibio-fibular socket or tibio-fibular mortise.
Below upper surface of body of talus, medially comma shaped facet for medial malleolus and laterally triangular facet of talus for lateral malleolus
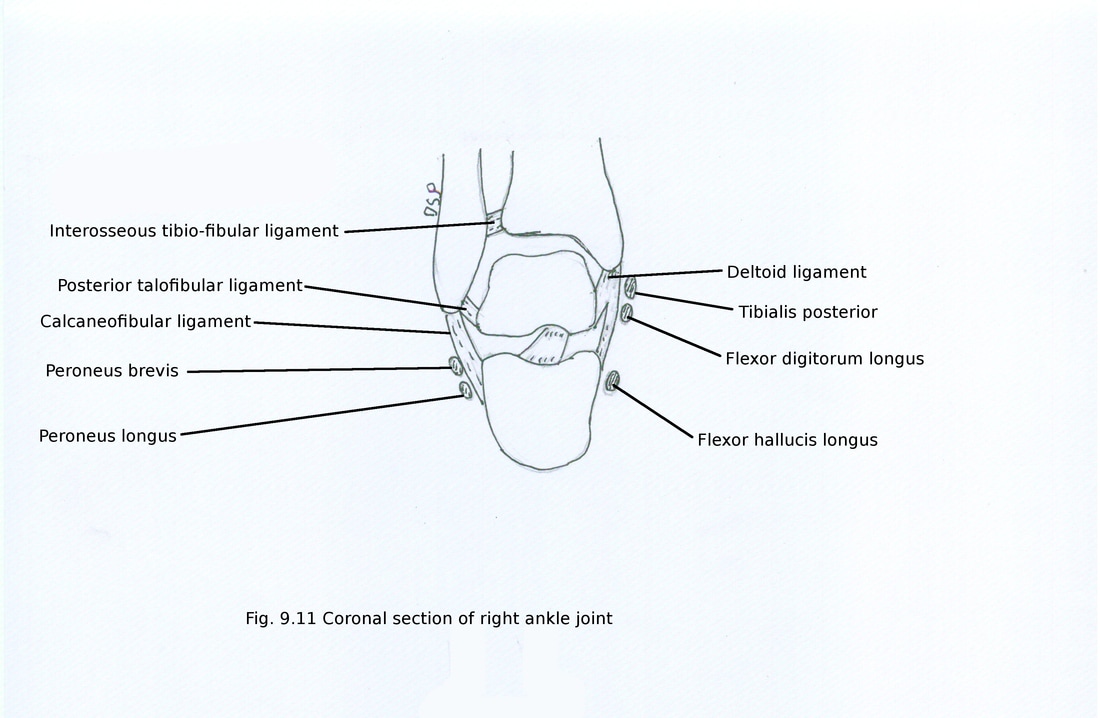
Ligaments :
1. Capsule : Above capsule shows attachment on lower end of tibia and fibula on margins of tibio-fibular mortise. Below it shows attachment on trochlea tali with extension on neck of talus on its dorsal surface. Capsule is thin in front and behind to allow movement at joint. Synovial membrane present on inner surface of capsule but it shows upward extension in inferior tibio-fibular joint and membrane not present in relation with articular cartilage.
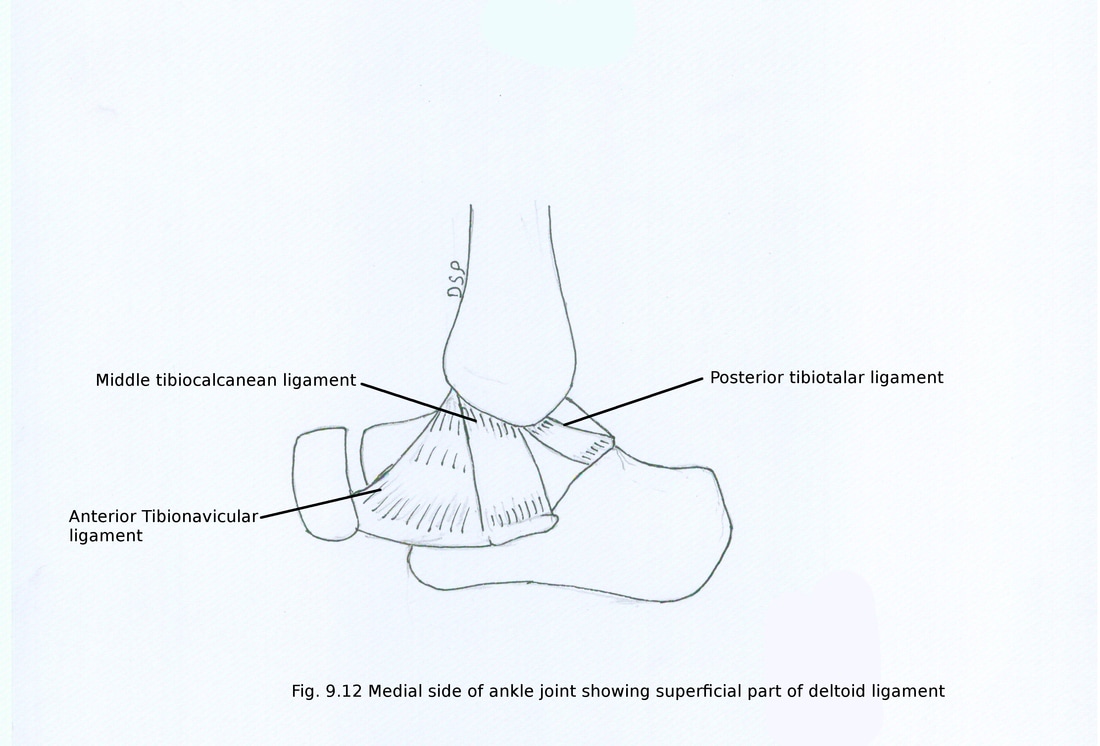
2. Deltoid ligament : It is a strong triangular ligament present on medial aspect of joint. It shows two parts superficial and deep. Superficial part shows attachment above on apex and margins of medial malleolus. Superficial part shows again three parts anterior, middle and posterior. Anterior part goes downward and forward. It shows attachment below on tuberosity of navicular bone. Middle part goes downward and shows attachment on sustentaculum tali of calcaneus bone. Posterior part goes downward and backward shows attachment on medial tubercle and medial surface of talus.
Deep part shows attachment on medial malleolus near tip and anterior part of medial surface of talus. Deltoid ligament crossed superficially by tendons of tibialis posterior and flexor digitorum longus.
1. Capsule : Above capsule shows attachment on lower end of tibia and fibula on margins of tibio-fibular mortise. Below it shows attachment on trochlea tali with extension on neck of talus on its dorsal surface. Capsule is thin in front and behind to allow movement at joint. Synovial membrane present on inner surface of capsule but it shows upward extension in inferior tibio-fibular joint and membrane not present in relation with articular cartilage.
2. Deltoid ligament : It is a strong triangular ligament present on medial aspect of joint. It shows two parts superficial and deep. Superficial part shows attachment above on apex and margins of medial malleolus. Superficial part shows again three parts anterior, middle and posterior. Anterior part goes downward and forward. It shows attachment below on tuberosity of navicular bone. Middle part goes downward and shows attachment on sustentaculum tali of calcaneus bone. Posterior part goes downward and backward shows attachment on medial tubercle and medial surface of talus.
Deep part shows attachment on medial malleolus near tip and anterior part of medial surface of talus. Deltoid ligament crossed superficially by tendons of tibialis posterior and flexor digitorum longus.
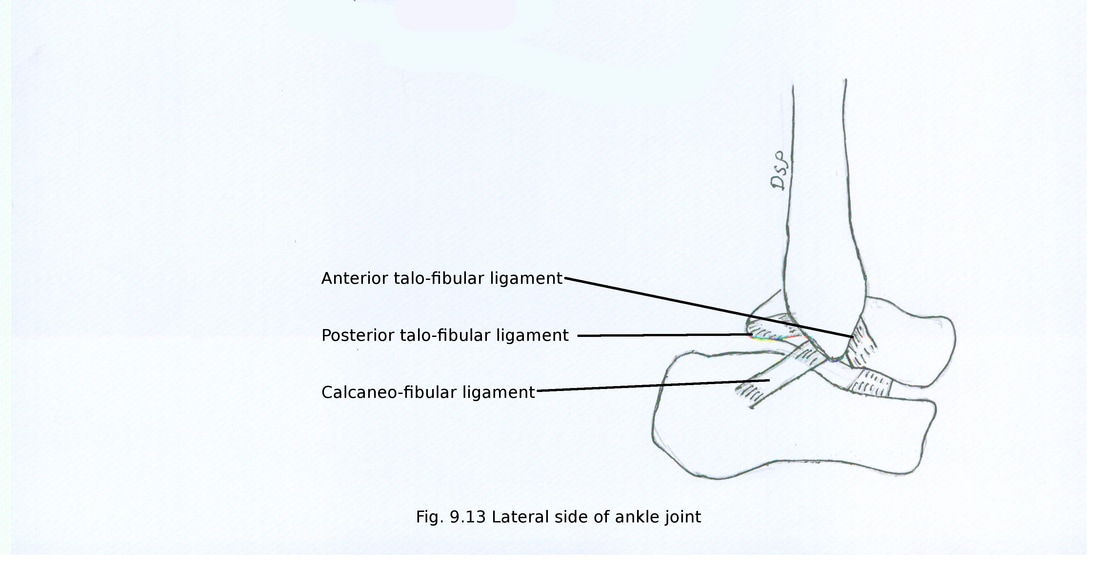
3. Lateral ligament : These are three in number anterior talo-fibular, posterior talo-fibular and calcaneo-fibular. Anterior talo-fibular ligament goes antero-medially shows attachment on anterior margin of lateral malleolus and lateral surface of neck of talus. Posterior talo-fibular ligament goes posteriorly shows attachment on posterior margin of lateral malleolus near lateral malleolar fossa and posterior tubercle of talus. Calcaneo-fibular ligament goes downward shows attachment on tip of lateral malleolus and tubercle on lateral surface of calcaneus. It is superficially crossed by peroneus longus and peroneus brevis muscle.
Relations :
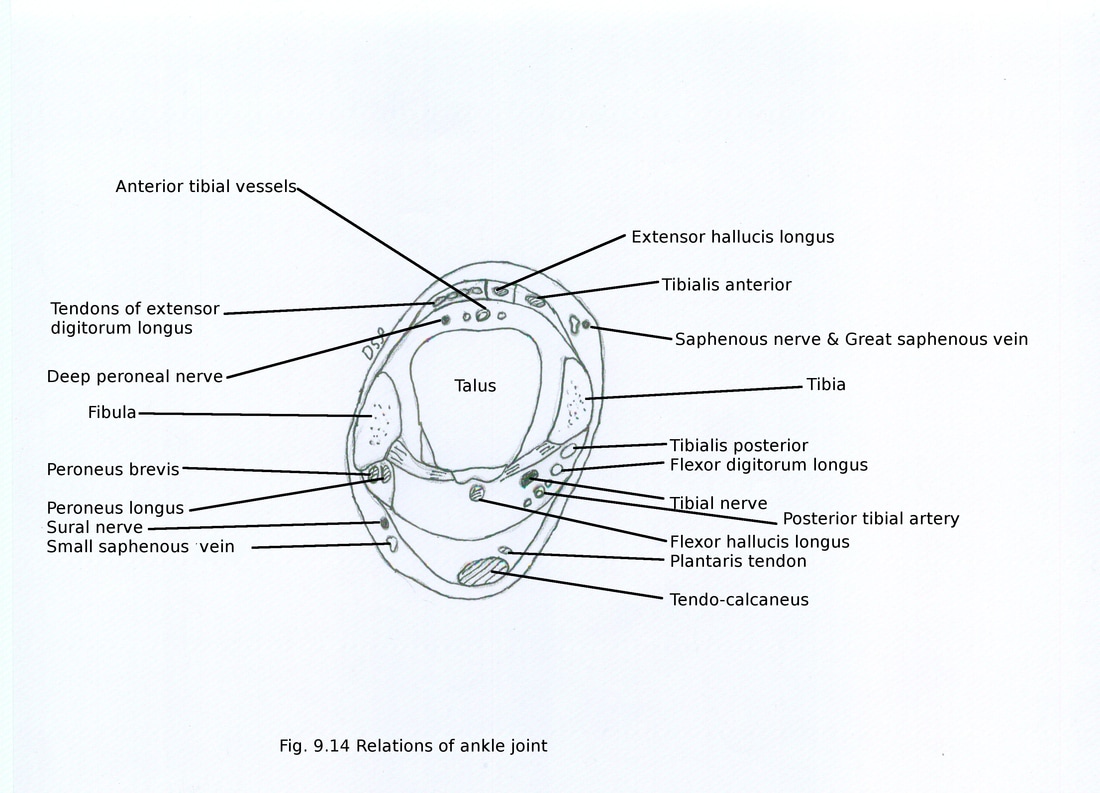
Anteriorly: From medial to lateral side following structures are related. Tendon of tibialis anterior, extensor hallucis longus, anterior tibial vessels, deep peroneal nerve, extensor digitorum longus, peroneus tertius.
Posteriorly : Tendo -calcaneus present exact posteriorly. In relation with medial malleolus structures present from medial to lateral side are tendon of tibialis posterior, flexor digitorum longus, posterior tibial vessels, tibial nerve, flexor hallucis longus. In relation with lateral malleolus deep tendon of peroneus brevis and superficial tendon of peroneus longus
Anteriorly: From medial to lateral side following structures are related. Tendon of tibialis anterior, extensor hallucis longus, anterior tibial vessels, deep peroneal nerve, extensor digitorum longus, peroneus tertius.
Posteriorly : Tendo -calcaneus present exact posteriorly. In relation with medial malleolus structures present from medial to lateral side are tendon of tibialis posterior, flexor digitorum longus, posterior tibial vessels, tibial nerve, flexor hallucis longus. In relation with lateral malleolus deep tendon of peroneus brevis and superficial tendon of peroneus longus
Blood Supply: It is supplied by malleolar branches of anterior and posterior tibial artery and peroneal artery.
Nerve supply: It is supplied by branches of deep peroneal nerve, tibial nerve, saphenous nerve and sural nerve.
Muscles for movements :
Two types of movements seen at ankle joint dorsi-flexion and plantar-flexion. In dorsi-flexion angle between leg and dorsum of foot decreases. In plantar-flexion angle between leg and dorsum of foot increases. Dorsi-flexion takes place up to 10 degree can be increased passively up to 20 degree. Plantar-flexion takes place up to 20 degree but can be increased up to 40 degree.
Dorsi-Flexion : It is produced by tibialis anterior, extensor digitorum longus, extensor hallucis longus and peroneus tertius.
Plantar-Flexion : It is mainly produced by gastrocnemius and soleus. These are assisted by plantaris, tibialis posterior, flexor digitorum longus and flexor hallucis longus.
Applied anatomy :
1. Sprain : It is a condition in which stretching or tearing of ligaments occur. Ankle sprain anterior talo-fibular and calcaneo-fibular ligaments are affected during inversion and plantar-flexion of foot.
2. Pott’s fracture : In forceful eversion of foot avulsion fracture (horizontal fracture) of medial malleolus occurs with fracture of shaft of fibula (oblique fracture) slightly above ankle joint.
Nerve supply: It is supplied by branches of deep peroneal nerve, tibial nerve, saphenous nerve and sural nerve.
Muscles for movements :
Two types of movements seen at ankle joint dorsi-flexion and plantar-flexion. In dorsi-flexion angle between leg and dorsum of foot decreases. In plantar-flexion angle between leg and dorsum of foot increases. Dorsi-flexion takes place up to 10 degree can be increased passively up to 20 degree. Plantar-flexion takes place up to 20 degree but can be increased up to 40 degree.
Dorsi-Flexion : It is produced by tibialis anterior, extensor digitorum longus, extensor hallucis longus and peroneus tertius.
Plantar-Flexion : It is mainly produced by gastrocnemius and soleus. These are assisted by plantaris, tibialis posterior, flexor digitorum longus and flexor hallucis longus.
Applied anatomy :
1. Sprain : It is a condition in which stretching or tearing of ligaments occur. Ankle sprain anterior talo-fibular and calcaneo-fibular ligaments are affected during inversion and plantar-flexion of foot.
2. Pott’s fracture : In forceful eversion of foot avulsion fracture (horizontal fracture) of medial malleolus occurs with fracture of shaft of fibula (oblique fracture) slightly above ankle joint.
OTHER JOINTS OF FOOT
Subtalar, transverse tarsal or mid-tarsal, intertarsal, intermetatarsal, tarso-metatarsal, metatarso-phalangeal, interphalangeal joints are present in between bones of foot.
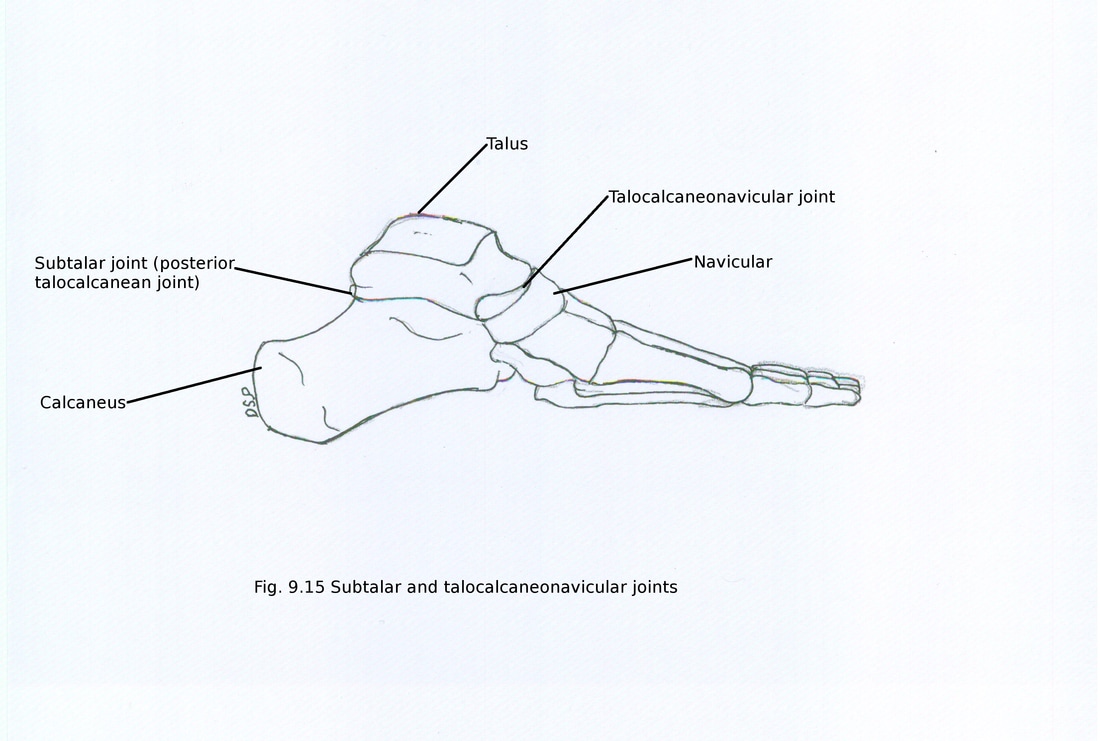
SUBTALAR JOINT (POSTERIOR TALO-CALCANEAN JOINT)
It is plane type of joint.
Bones forming joints :
It is formed between concave facet of lower surface of body of talus and convex facet on middle third of calcaneus.
Ligaments : These are 1) Capsule 2) Lateral talo-calcanean ligament 3) Medial talo-calcanean ligament 4) Interosseous talo-calcanean ligament 5) Cervical ligament.
1) Capsule : Capsule shows attachment on articular margins and envelops joint.
2) Lateral talo-calcanean ligament : It shows short fasciculi which descends oblique backward from lateral talar process to lateral calcaneal surface.
3) Medial talo-calcanean ligament : It connects medial tubercle of talus to back of sustentaculum tali and medial surface of calcaneus. It merges with deltoid ligament.
4) Interosseous talo-calcanean ligament : It fills up gap in sinus tarsi. It is broad, flat and bilaminar band. Bilaminar band shows anterior and posterior lamina. Anterior lamina associated with talocalcaneonavicular joint and posterior lamina with talo-calcanean joint. Medial part becomes taut in eversion.
5) Cervical ligament : It connects upper surface of calcaneus with lateral surface of neck of talus. It becomes taut in inversion.
Nerve supply: It is supplied by branches of posterior tibial, sural and medial plantar nerve.
Subtalar, transverse tarsal or mid-tarsal, intertarsal, intermetatarsal, tarso-metatarsal, metatarso-phalangeal, interphalangeal joints are present in between bones of foot.
SUBTALAR JOINT (POSTERIOR TALO-CALCANEAN JOINT)
It is plane type of joint.
Bones forming joints :
It is formed between concave facet of lower surface of body of talus and convex facet on middle third of calcaneus.
Ligaments : These are 1) Capsule 2) Lateral talo-calcanean ligament 3) Medial talo-calcanean ligament 4) Interosseous talo-calcanean ligament 5) Cervical ligament.
1) Capsule : Capsule shows attachment on articular margins and envelops joint.
2) Lateral talo-calcanean ligament : It shows short fasciculi which descends oblique backward from lateral talar process to lateral calcaneal surface.
3) Medial talo-calcanean ligament : It connects medial tubercle of talus to back of sustentaculum tali and medial surface of calcaneus. It merges with deltoid ligament.
4) Interosseous talo-calcanean ligament : It fills up gap in sinus tarsi. It is broad, flat and bilaminar band. Bilaminar band shows anterior and posterior lamina. Anterior lamina associated with talocalcaneonavicular joint and posterior lamina with talo-calcanean joint. Medial part becomes taut in eversion.
5) Cervical ligament : It connects upper surface of calcaneus with lateral surface of neck of talus. It becomes taut in inversion.
Nerve supply: It is supplied by branches of posterior tibial, sural and medial plantar nerve.
TRANSVERSE TARSAL OR MID-TARSAL JOINTS
Two joints are included in it 1) Talocalcaneonavicular joint 2) Calcaneocuboid joint.
1) TALOCALCANEONAVICULAR JOINT
It ball and socket type of joint.
Bones and structures forming joints :
It is formed between convex ovoid head of talus articulating with socket formed by concave posterior surface of navicular bone, middle and anterior facet of calcaneus, superior surface of plantar calcaneonavicular ligament (spring ligament).
Ligaments :
Ligaments of the joint are capsule, talonavicular and plantar calcaneonavicular.
Capsule is weak but posteriorly thick. Synovial cavity of it shows communication with cavity of talocalcaneal joint.
Talonavicular ligament connecting dorsal part of neck of talus and navicular bone.
Plantar calcaneonavicular (spring) ligament connecting navicular bone with anterior margin of sustentaculum tali on plantar aspect. It supports head of talus from below. Fibro-cartilagenous tissues present in relation with upper part of ligament. Medially it is continuous with superficial fibres of deltoid ligament and laterally with short plantar ligament. Below it is supported by tendons of tibialis posterior, flexor hallucis longus and flexor digitorum longus mediolaterally.
Nerve supply: It is supplied by branches of deep peroneal and medial plantar nerve.
2) CALCANEOCUBOID JOINT
It is a transverse tarsal joint of saddle variety.
Bones and structures forming joints :
It is formed between anterior surface of calcaneus and posterior surface of cuboid.
Ligaments :
Ligaments of the joint are capsule, bifurcate ligament, long plantar ligament and plantar calcaneocuboid ligament.
Capsule : It covers joint and dorsally thickened by dorsal calcaneocuboid ligament.
Bifurcate ligament : It is Y shaped. Stem of Y shows attachment on anterior part of upper surface of calcaneus. Two limbs diverge anteriorly and shows shows attachment medially on dorsolateral aspect of navicular bone as calcaneonavicular ligament and laterally on dorsomedial aspect of cuboid bone as calcaneocuboid ligament.
Long plantar ligament : It is the longest ligament. It shows attachment on plantar surface of calcaneus on a triangular area between anterior and two posterior tubercles to a oblique ridge on plantar surface of cuboid. Superficial fibres make a tunnel on cuboid for the tendon of peroneus longus and shows attachment on second, third fourth and sometimes fifth metatarsal bones.
Short plantar ligament (Plantar calcaneocuboid ligament) : It is a short ligament deep to long plantar ligament. It shows attachment on anterior tubercle of calcaneus and plantar surface of cuboid bone posterior to oblique ridge.
Nerve supply: It is supplied by branches of sural, deep peroneal and lateral plantar nerve.
INTERTARSAL JOINTS
These are joints between three cuneiform bones (intercuneiform), between lateral cuneiform and cuboid bone (cuneocuboid). All these are plane synovial type.
INTERMETATARSAL JOINTS
These are joints between adjacent surface of base of the second, third and fourth metatarsal bones.
TARSO-METATARSAL JOINTS
These are plane synovial type. These are joints between medial cuneiform with base of the first metatarsal, intermediate and lateral cuneiform with base of the second, third metatarsal bones, cuboid bone with fourth and fifth metatarsal bones. Ligaments present in relation with these joints are capsule, dorsal, plantar tarsometatarsal and interosseous cuneometatarsal ligament.
Movements : Following movements takes place at these joints are flexion and extension but in first tarsometatarsal abduction and rotation occurs.
Nerve supply: It is supplied by branches of deep peroneal nerve, medial two joints by medial plantar nerve and lateral joints are by lateral plantar nerve.
METATARSO-PHALANGEAL JOINTS
These are ellipsoid type of synovial joint. These are joints between convex head of metatarsal with concave base of proximal phalanx. Ligaments present in relation with these joints are capsule, plantar, collateral and deep transverse metatarsal ligament.
Movements : Following movements takes place at these joints are dorsi-flexion (50-60 degree), plantar-flexion (30-40 degree), adduction and abduction.
INTERPHALANGEAL JOINTS
These are hinge type of joints. These are joints between head of phalanges with base of phalanges. Two types proximal and distal interphalangeal joints are present. Ligaments present in relation with these joints are capsule, two collateral ligament.
Movements : Following movements takes place at these joints are flexion and extension. Flexion is produced by flexor digitorum longus, flexor digitorum brevis, flexor hallucis longus and flexor accessorius. Extension is produced by extensor digitorum longus, extensor digitorum brevis and extensor hallucis longus.
Nerve supply: It is supplied by branches of plantar interdigital nerve, dorsal cutaneous branch of superficial peroneal, deep peroneal, sural nerve.
INVERSION AND EVERSION OF FOOT
In inversion of foot medial border of foot raised and sole facing medially downward. During inversion also plantar flexion takes place. In eversion of foot lateral border of foot raised and sole facing laterally downward. During eversion also dorsi flexion takes place. These movements are best visible when foot is off the ground.
During inversion of foot anterior part of foot get adducted at mid-tarsal joint then lateral rotation takes place at subtalar joint. During eversion of foot anterior part of foot get abducted at mid-tarsal joint then medial rotation takes place at subtalar joint.
Joints involved : Subtalar and transverse tarsal or midtarsal (talocalcaneonavicular, calcaneocuboid) joints are involved.
Axis for this movement passes upward, forward and medially from back of calcaneus through sinus tarsi to dorsomedial surface of neck of talus.
Inversion can take place up to 30 degree and eversion can take place up to 20 degree.
Muscles for movements :
For inversion tibialis anterior, tibialis posterior assisted by flexor hallucis longus, flexor digitorum longus. For eversion peroneus longus, peroneus brevis assisted by peroneus tertius.
These movements are important for adjustment of foot on uneven ground.
Two joints are included in it 1) Talocalcaneonavicular joint 2) Calcaneocuboid joint.
1) TALOCALCANEONAVICULAR JOINT
It ball and socket type of joint.
Bones and structures forming joints :
It is formed between convex ovoid head of talus articulating with socket formed by concave posterior surface of navicular bone, middle and anterior facet of calcaneus, superior surface of plantar calcaneonavicular ligament (spring ligament).
Ligaments :
Ligaments of the joint are capsule, talonavicular and plantar calcaneonavicular.
Capsule is weak but posteriorly thick. Synovial cavity of it shows communication with cavity of talocalcaneal joint.
Talonavicular ligament connecting dorsal part of neck of talus and navicular bone.
Plantar calcaneonavicular (spring) ligament connecting navicular bone with anterior margin of sustentaculum tali on plantar aspect. It supports head of talus from below. Fibro-cartilagenous tissues present in relation with upper part of ligament. Medially it is continuous with superficial fibres of deltoid ligament and laterally with short plantar ligament. Below it is supported by tendons of tibialis posterior, flexor hallucis longus and flexor digitorum longus mediolaterally.
Nerve supply: It is supplied by branches of deep peroneal and medial plantar nerve.
2) CALCANEOCUBOID JOINT
It is a transverse tarsal joint of saddle variety.
Bones and structures forming joints :
It is formed between anterior surface of calcaneus and posterior surface of cuboid.
Ligaments :
Ligaments of the joint are capsule, bifurcate ligament, long plantar ligament and plantar calcaneocuboid ligament.
Capsule : It covers joint and dorsally thickened by dorsal calcaneocuboid ligament.
Bifurcate ligament : It is Y shaped. Stem of Y shows attachment on anterior part of upper surface of calcaneus. Two limbs diverge anteriorly and shows shows attachment medially on dorsolateral aspect of navicular bone as calcaneonavicular ligament and laterally on dorsomedial aspect of cuboid bone as calcaneocuboid ligament.
Long plantar ligament : It is the longest ligament. It shows attachment on plantar surface of calcaneus on a triangular area between anterior and two posterior tubercles to a oblique ridge on plantar surface of cuboid. Superficial fibres make a tunnel on cuboid for the tendon of peroneus longus and shows attachment on second, third fourth and sometimes fifth metatarsal bones.
Short plantar ligament (Plantar calcaneocuboid ligament) : It is a short ligament deep to long plantar ligament. It shows attachment on anterior tubercle of calcaneus and plantar surface of cuboid bone posterior to oblique ridge.
Nerve supply: It is supplied by branches of sural, deep peroneal and lateral plantar nerve.
INTERTARSAL JOINTS
These are joints between three cuneiform bones (intercuneiform), between lateral cuneiform and cuboid bone (cuneocuboid). All these are plane synovial type.
INTERMETATARSAL JOINTS
These are joints between adjacent surface of base of the second, third and fourth metatarsal bones.
TARSO-METATARSAL JOINTS
These are plane synovial type. These are joints between medial cuneiform with base of the first metatarsal, intermediate and lateral cuneiform with base of the second, third metatarsal bones, cuboid bone with fourth and fifth metatarsal bones. Ligaments present in relation with these joints are capsule, dorsal, plantar tarsometatarsal and interosseous cuneometatarsal ligament.
Movements : Following movements takes place at these joints are flexion and extension but in first tarsometatarsal abduction and rotation occurs.
Nerve supply: It is supplied by branches of deep peroneal nerve, medial two joints by medial plantar nerve and lateral joints are by lateral plantar nerve.
METATARSO-PHALANGEAL JOINTS
These are ellipsoid type of synovial joint. These are joints between convex head of metatarsal with concave base of proximal phalanx. Ligaments present in relation with these joints are capsule, plantar, collateral and deep transverse metatarsal ligament.
Movements : Following movements takes place at these joints are dorsi-flexion (50-60 degree), plantar-flexion (30-40 degree), adduction and abduction.
INTERPHALANGEAL JOINTS
These are hinge type of joints. These are joints between head of phalanges with base of phalanges. Two types proximal and distal interphalangeal joints are present. Ligaments present in relation with these joints are capsule, two collateral ligament.
Movements : Following movements takes place at these joints are flexion and extension. Flexion is produced by flexor digitorum longus, flexor digitorum brevis, flexor hallucis longus and flexor accessorius. Extension is produced by extensor digitorum longus, extensor digitorum brevis and extensor hallucis longus.
Nerve supply: It is supplied by branches of plantar interdigital nerve, dorsal cutaneous branch of superficial peroneal, deep peroneal, sural nerve.
INVERSION AND EVERSION OF FOOT
In inversion of foot medial border of foot raised and sole facing medially downward. During inversion also plantar flexion takes place. In eversion of foot lateral border of foot raised and sole facing laterally downward. During eversion also dorsi flexion takes place. These movements are best visible when foot is off the ground.
During inversion of foot anterior part of foot get adducted at mid-tarsal joint then lateral rotation takes place at subtalar joint. During eversion of foot anterior part of foot get abducted at mid-tarsal joint then medial rotation takes place at subtalar joint.
Joints involved : Subtalar and transverse tarsal or midtarsal (talocalcaneonavicular, calcaneocuboid) joints are involved.
Axis for this movement passes upward, forward and medially from back of calcaneus through sinus tarsi to dorsomedial surface of neck of talus.
Inversion can take place up to 30 degree and eversion can take place up to 20 degree.
Muscles for movements :
For inversion tibialis anterior, tibialis posterior assisted by flexor hallucis longus, flexor digitorum longus. For eversion peroneus longus, peroneus brevis assisted by peroneus tertius.
These movements are important for adjustment of foot on uneven ground.
